November Articles-Author Questions
Copyright © January 2006 Ted Nissen
TABLE OF
CONTENTS
1 What other research studies
have followed this one and have added to our knowledge of subacute low-back pain?
If you have pdf files please forward. 3
2 Can we get charts and other ancillary
material depicting/describing stretches/postural education massage techniques
used in this study? 3
3 Are copies of tests used in
the study available? For example; Roland
Disability Questionnaire (RDQ), McGill Pain Questionnaire (LF-MPQ) Long
Form, State-Trait Anxiety Inventory Form Y (STAI), & Modified Schober test. 3
4 Were the distributions of the
individual groups and combined scores of all the groups normal or skewed
negative/positive? 3
5 Outcome Measures for this
study indicate P-Values at follow-up of .04 between the Modified Schober Groups (Significant Differences between Groups) but .51
post treatment (No Difference). Since this may indicate a treatment effect
between groups at follow-up why didn’t you report this? Did you complete
further factor analysis to determine which groups were affected? What does it
mean? 3
6 What
was the funding source for this project? How much was the funding grant for?
Were the subjects paid and if so how much? When you (author) provided treatment
in the place of an unavailable massage therapist were you paid and what
percentage of treatment did you provide? 4
7 How
were the treatment providers selected? 4
8 Pedro (Physiotherapy Evidence Database) rates this
research as follows; 6 out of 10 possible (see Pedro Validity Standards). None of the following research elements were noted; Concealed
Allocation, Blind Subjects, Blind Therapists, and Intention to treat analysis.
Do you agree with Pedro’s analysis? 5
9 Please
clarify the apparent discrepancy between these two research findings from your
study; 5
10 At
follow-up the soft-tissue manipulation group (Group # 2) was not
distinguishable from Group 3 (exercise group). If this is true how can Group 1
be statistically superior to group 3 (also a finding in the study) since there
are no statistical differences between group 1 and group 2 at follow-up? 6
11 Why did the author find it
necessary to mention “College of Massage Therapists” in her summary conclusion
when regulation of massage technique & the experience of the massage
therapists are not measured variables in this research? 6
12 I can find no reference , which determines the validity of using the
PPI McGill pain scale, which is essentially an ordinal scale as a ratio scale
(used in your study to determine percentage of subjects with no pain). The
McGill appears to have been validated as an interval scale. Please let me know
if you have additional references? 6
13 Several comparisons between
groups, both at post treatment and at follow-up, were not mentioned in this
research paper. These are listed in the following chart in parenthesis; Outcome Measures
Results Can we assume that this is
because there are no significant differences between these groups? 7
Research
Article: Preyde M. Effectiveness of massage therapy for subacute low-back pain:
a randomized controlled trial. CMAJ 2000;162(13):1815-20.
Online
Article: http://www.cmaj.ca/cgi/reprint/162/13/1815
1.1 Authors Response
1.1.1 I have conducted
no further studies on treatment for subacute low back pain.
2.1 Authors Response
2.1.1 I do not have
these readily available.
2.2 Analysis
2.2.1 This is
unfortunate, given that the author makes the claim in question # 11 of this
paper that the results are not generalizable to other therapies which may seem similar.
The descriptions in the research paper are sketchy and do not distinguish these
techniques from those used in other settings. It is impossible to fully
evaluate the author’s claim without further demonstration of the technique as
requested in this question. The author is asking us to trust that this is so.
3.1 Authors Response
3.1.1 Yes, these
measures are readily available; however, one must purchase the Anxiety
Inventory.
4.1 Authors Response
4.1.1 The distributions
were normal.
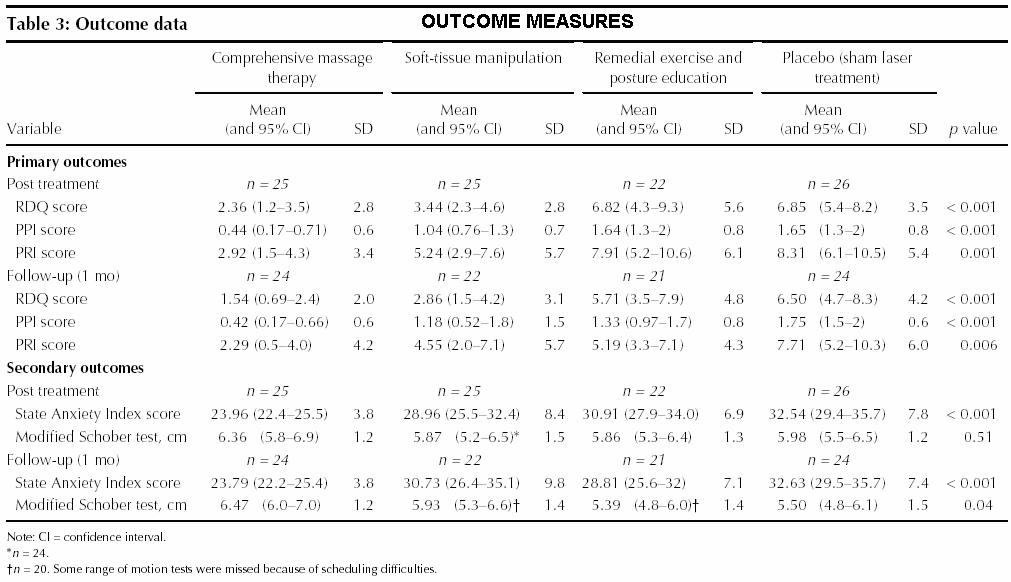
5
Outcome
Measures
for this study indicate P-Values at follow-up of .04 between the Modified Schober Groups (Significant
Differences between Groups) but .51 post treatment (No Difference). Since this
may indicate a treatment effect between groups at follow-up why didn’t you
report this? Did you complete further factor analysis to determine which groups
were affected? What does it mean?
5.1 Authors Response
5.1.1 This is a good
question. This result was reported in Table 3, but not discussed. While it
appears that the participants in the comprehensive massage therapy group had
the greatest range of motion at one-month follow up, you might note that due to
scheduling difficulties, not all the participants in the soft tissue
manipulation group underwent this test. I therefore did not have confidence in
this finding especially since the sample sizes were somewhat small. As you know, there are revisions and editions
requested by journal editors and pressure to streamline the manuscript – not
everything in the first manuscript submission appears in the published version.
6.1 Authors Response
6.1.1 As noted in the
article, the College of Massage Therapists funded the study ($38,000). When I
provided treatment which was rare (perhaps 1-2%), I did not reimburse myself.
7.1 Authors Response
7.1.1 At the time of the
study, the study site was new and still in the process of becoming fully
developed. The coordinator of the Centre had recently interviewed several
people for the Centre, and this coordinator assisted with locating appropriate
personnel for the study.
7.2 Analysis
7.2.1
8
Pedro (Physiotherapy Evidence Database) rates this
research as follows; 6 out of 10 possible (see Pedro Validity Standards). None of the
following research elements were noted; Concealed Allocation, Blind Subjects,
Blind Therapists, and Intention to treat analysis. Do you agree with Pedro’s
analysis?
8.1
Authors Response
8.1.1 This is not
entirely correct. Data were analyzed by intention to treat.
8.1.2 It would be
difficult if not impossible to blind subjects and therapists to treatment
allocation; however, subjects were blind to purpose and the use of a placebo.
8.2 Analysis
8.2.1 Pedro is not clear
about how they determine whether statistical analysis (Intention to Treat
Analysis) was done on treatment variables even though a person dropped out of
the study before completion. Pedro cites the research link below which seems to
require explicit description and intention to treat analysis included in the research
paper. It may be that you don’t get credit unless you clearly say that you
analysed all of the outcome measures even if someone dropped out. In this case
this study does not detail a description of the intention to treat analysis and
so despite the authors current claim that intention to treat analysis was
performed it has to be documented clearly in the research which was not done.
The author is asking us to trust that she performed the intention to treat
analysis without any material demonstration that this analysis was in fact
done.
8.2.2
Intention to Treat Research cited
by Pedro
8.2.3
The author states that it “would be
difficult if not impossible to blind subjects and therapists to treatment
allocation”. The term allocation concealment technically applies only to the
screener’s inability to see the allocation of subjects to groups by the
assignment person. The author seems to confuse this term “concealed allocation”
with blinding therapists that is insuring that therapists don’t know which
groups are supposed to be therapeutic. The author conflates these two terms
into one term “treatment allocation” claiming it to be impractical. We will
pull these two terms apart and deal with them separately as this is a mistaken
use of the term by the researcher.
8.2.4
In this study there was no
description of procedures for allocation concealment (Definition). There are
several accepted and well established measures which effectively conceal
allocation (Proceedures). The researchers
claim that allocation concealment is difficult/impossible is simply not true.
The author could be ignorant of basic research and design methodology which
seems implausible given her current active involvement as a research professor
at a prominent Canadian University. This author could also be attempting to
spin (misleading
interpretation of material facts and or introduction of irrelevant information
to argue in support of a false conclusion) a defence for what is an obvious design flaw in the research.
8.2.5
There is other evidence of spin on
the part of the researcher in defending this study. (spin) There may be other
explanations for this behavior which should be considered given the affect that
this particular description would have on the reader’s ability to trust the
judgements and recollections of the researcher.
8.2.6
After all how trust worthy is a
person who knowingly misleads readers into supporting a false conclusion? How
would you know what was true and what wasn’t? In some instances you have to
take the researchers word for information which is unverifiable. For example
this researcher has claimed that the distribution of the data for this research
study are normal (this might allow us to verify bias), that she only saw
patients 1-2% of the time, did not get paid for her service, had no personal
relationships with the therapists who provided research in the study and other
material facts which would affect the validly of research conclusions.
8.2.7
How can we trust that these
material facts are correct if there is evidence of spin? Spin by definition
implies a misleading interpretation of material facts. What is truth and what
isn’t becomes a valid concern with this research. It certainly is possible that
the author is telling the truth about some things and spinning others. Whether
these are outright lies or if there is actual fraud is impossible to tell.
8.2.8
The advice to researchers is
simple; defend your position where possible but it is probably better to admit
error rather than sacrifice trust. In the long run it is likely that people
will see thru half truths and misleading arguments and not trust any of the
conclusions of the research study. The short term benefit to reputation that
spinning away embarrassing research errors may provide is offset by the long
term mistrust of research findings. It certainly isn’t worth it to the funding
source if no one trusts the research they financially sponsor.
8.2.9
The second assertion that it is
difficult or impossible to blind therapists may be true. It will require more
research to determine whether creative solutions to this problem have been
devised. How would you blind therapists or for that matter subjects to which of
the groups had the measured treatment? The blinding technique is well suited
for drug therapies where a placebo pill is made to look like the real pill. How
do you make it difficult/impossible for both therapist and subject to know
which therapeutic intervention is real? Most massage therapists/subjects would
be suspicious for example if you tried to sell a sham (fake) therapeutic
intervention that was applied to a different area of the body than the problem
area. Then again how would you avoid an unwanted treatment effect if you did
apply treatment to the affected area? This problem may have been resolved
already and it will be interesting to see how.
8.2.10 This does not mean that this research or any research in the field of
touch therapy should be exempted from rating this good research criterion. It
will hopefully motivate researchers to develop creative solutions which blind
both therapists and subjects to insure that they are not influencing the
outcome of the research and the therapeutic intervention is. The excuse that
this researcher promotes that it is difficult or impossible would probably not
be acceptable to the scientific community.
9.1 At the 1-month follow-up, 63% of the subjects
in the comprehensive massage therapy group reported no pain, as compared with
27% in the soft-tissue manipulation group…
9.2 At follow-up there
were no statistical differences between the comprehensive massage therapy group
and the soft-tissue manipulation group
9.3 Authors Response
9.3.1 At follow-up the
soft-tissue manipulation group (Group # 2) was not distinguishable from Group 3
(exercise group). If this is true how can Group 1 be statistically superior to
group 3 (also a finding in the study) since there are no statistical
differences between group 1 and group 2 at follow-up?
10.1 Authors Response
10.1.1 The difference
between group 2 and 3 was not statistically significant, while the difference
between group 1 and 3 was statistically significant.
11.1
Authors Response
11.1.1 I do not see
College of MT in the summary conclusion. It is important to note that the
effectiveness suggested in this study is only associated with comprehensive
massage therapy by experienced therapists with additional training, and so
forth as noted in the article. The findings are not generalizable to other form
of therapies that one might consider similar.
11.2 Analysis
11.2.1 The author could
find the reference if she had looked. For your convenience it is highlighted
with the following link.
11.2.2 It does appear to
be a blatant plug of the college of massage therapists which funded this
research project and of which she was registered. This plug may be hard to
defend if she had acknowledged awareness of it. The author seems to want to
defend her inclusion of the plug without acknowledging its existence. Ms.
Preyde asserts that the additional training and experience of the massage
therapists providing treatment in her study did affect the quality of service
provision. Ms. Preyde further asserts that the superior outcome that
comprehensive massage therapy affords can not be generalized to treatments
which may only seem similar. Ms.
Preyde’s aforementioned conclusion is not supported by the evidence and is
irrelevant to the variables measured in this research. This research study does
not measure the experience of therapists, the amount of training they received,
what institution registered them or how those variables in combination affected
the administration of the measured variable comprehensive massage. In addition at least a part of the
comprehensive massage treatments were not provided by massage therapists but
rather a certified personal trainer/weight-trainer supervisor whose experience
or training is not known. This appears to be some type of spin (misleading
interpretation of facts to the advantage of a premise) on the part of Ms.
Preyde which avoids taking responsibility for an error in judgement or worse is
just a reasoned and conscious intent to deceive. Ms. Preyde should not have
inserted the plug in the first place. The spin that Ms. Preyde advances assumes
ignorance and lack of scientific sophistication on the part of the reader. It
seems obvious Ms. Preyde intends to manipulate our perception of this study so
that we may favour the college of massage therapists as a training institution.
This casts unnecessary doubt on her other recollections or analysis. How can
we, the reader, trust Ms. Preyde recollections and answers to other questions
when something she denies seeing is in such plain sight and further something
she defends anyway as if she knew it were there all along. We would have to
give her points for loyality and political savvy even at the expense of good
science.
12 I can find no
reference [1] [2] [3], which determines the validity of using the PPI McGill pain
scale, which is essentially an ordinal scale as a ratio scale (used in your study
to determine percentage of subjects with no pain). The McGill appears to have
been validated as an interval scale. Please let me know if you have additional
references?
12.1 Authors Response
12.1.1 I am sorry, I do
not have other references.
12.2 Analysis
12.2.1
13.1 Authors Response
13.1.1 I think the
important statistically significant differences were noted in the article.
[1]
Prieto Ej, Hopson L, Bradley La, Byrne M, Geisinger Kf, Midax D, Et Al. (Feb
1980). The language of low back pain: factor structure of the mcgill pain
questionnaire. Pain, 8(1), pp. 11 - 19.
[2]
Mccreary C, Turner J, Dawson E. (Aug 1981). Principal dimensions of the pain
experience and psychological disturbance in chronic low back pain patients. Pain,
11(1), pp. 85 - 92.
[3]
Wright Kd, Asmundson Gj, Mccreary Dr. (2001). Factorial validity of the
short-form mcgill pain questionnaire (sf-mpq). Eur J Pain, 5(3), pp. 279
- 284.
{kind=link}
{kind=link}