Copyright Feb 2003 Ted Nissen.BEGIN1 END1
TABLE OF
CONTENTS
1 ABDUCTOR DIGITI MINIMI (FOOT)
2 ABDUCTOR DIGITI MINIMI (HAND)
4 ABDUCTOR POLLICIS BREVIS B4E4
5 ABDUCTOR POLLICIS LONGUS B5E5
13 BICEPS FEMORIS (Lateral
Hamstring) B13E13
17 BULBOCAVERNOSUS
(BULBOSPONGIOSUS) B17E17.
19 COCCYGEUS (ISCHIOCOCCYGEUS)
B19E19
21 CORRUGATOR SUPERCILII B21E21
22 CRICOARYTENOID LATERAL &
POSTERIOR B22E22
32 DIGASTRIC ANT & POST BELLY
(SUPRAHYOID)
36 EXTENSOR CARPI RADIALIS BREVIS
37 EXTENSOR CARPI RADIALIS LONGUS
48 EXTERNAL ABDOMINAL OBLIQUE=ANT
DIV
49 EXTERNAL ABDOMINAL OBLIQUE=LAT
DIV
52 EXTRINSIC AURICULAR MUSCLES
55 FLEXOR DIGITI MINIMI BREVIS
(FOOT)
56 FLEXOR DIGITI MINIMI BREVIS
(HAND)
60 FLEXOR DIGITORUM SUPERFICIALIS
67 GEMELLUS INFERIOR (1 of 6
Deep Lateral Rotators of Femur)
68 GEMELLUS SUPERIOR (1 of 6
Deep Lateral Rotators of Femur)
82 INFERIOR LONGITUDINAL LINGUALIS
84 INFERIOR PHARYNGEAL CONSTRICTOR
86 INFRASPINATUS (Rotator Cuff
Muscle)
87 INTERNAL ABDOMINAL OBLIQUE (Anterior
Division)
88 INTERNAL ABDOMINAL OBLIQUE
(Lateral Division)
92 INTRINSIC AURICULAR MUSCLES
98 LEVATOR ANGULI ORIS(CANINUS)
99 LEVATOR ANI, ILIAC
PART(ILIOCOCCYGEUS)
100 LEVATOR ANI, PUBIC
PART(PUBOCOCCYGEUS)
102 LEVATOR LABII SUPERIORIS ALAEQUE
NASI
103 LEVATOR PALPEBRAE SUPERIORIS
120 MIDDLE PHARYNGEAL CONSTRICTOR
125 NASALIS (COMPRESSOR & DILATOR
NARIS)
126 OBLIQUE ARYTENOID &
ARYEPIGLOTTICUS
129 OBTURATOR EXTERNUS (1 of 6
Deep Lateral Rotators of Femur)
130 OBTURATOR INTERNUS (1 of 6
Deep Lateral Rotators of Femur)
132 OMOHYOID SUPERIOR & INFERIOR
(INFRAHYOID)
137 PALATOGLOSSUS (Palatoglossal
arch; Anterior pillar)
138 PALATOPHARYNGEUS
(Palatopharyngeal arch; Posterior pillar)
143 PECTORALIS MAJOR CLAVICULAR
149 PIRIFORMIS (1 of 6 Deep
Lateral Rotators of Femur)
161 QUADRATUS FEMORIS (1 of 6 Deep
Lateral Rotators of the Femur)
164 RECTUS ABDOMINIS (4 Divisions as
1)
167 RECTUS CAPITIS POSTERIOR MAJOR
168 RECTUS CAPITIS POSTERIOR MINOR
169 RECTUS FEMORIS (Quadriceps
Femoris) (1 of 4 Quadriceps)
180 SEMIMEMBRANOSUS (Medial
Hamstring)
184 SEMITENDINOSUS (Medial
Hamstring)
186 SERRATUS POSTERIOR INFERIOR
187 SERRATUS POSTERIOR SUPERIOR
200 STERNOTHYROID (INFRAHYOID)
205 SUBSCAPULARIS (Rotator Cuff
Muscle)
206 SUPERFICIAL TRANSVERSE PERINEUS
(SUPERFICIALIS)
207 SUPERIOR LONGITUDINAL LINGUALIS
209 SUPERIOR PHARYNGEAL CONSTRICTOR
212 SUPRASPINATUS (Rotator Cuff
Muscle)
218 TERES MINOR (Rotator Cuff Muscle)
219 THYROARYTENOID VOCALIS &
THYROEPIGLOTTICUS
225 TRANSVERSE LINGUALIS (BODY OF
TONGUE)
226 TRANSVERSE PERINEUS (PROFUNDUS)
227 TRAPEZIUS LOWER (Lower Division)
232 VASTUS INTERMEDIUS (QUADRICEPS
FEMORIS) (1 of 4 Quadriceps)
233 VASTUS LATERALIS (Quadriceps
Femoris) (1 of 4 Quadriceps)
234 VASTUS MEDIALIS (Quadriceps
Femoris) (1 of 4 Quadriceps)
235 VERTICAL LINGUALIS (BODY OF
TONGUE)
1
ABDUCTOR DIGITI MINIMI (FOOT)
Back Table of Contents References
1.1 Word Derivation Pronounce
Pronounce
1.1.1 Abductor=Moves
part away from midline
1.1.2 Digit=Finger or
toe
1.1.3 Minimi= Little
finger or toe
1.2 Attachments Illus. (DSL)
1.2.1 Origin
1.2.1.1
Medial and lateral processes of the tuberosity of calcaneus
1.2.2 Insertion
1.2.2.1
Lateral side of the base of the proximal phalanx of the
fifth toe
1.3 Action Illus. (DSL)
1.3.1 Abducts
the fifth toe away from the fourth toe
1.4 Nerve Supply
1.4.1 Nerve
1.4.1.1
Lateral plantar nerve
1.4.2 Roots
1.4.2.1
S2
1.4.2.2
S3
1.5 Synergists
1.5.1 None
1.1 Muscle Tests
1.1.1 Abductor Digiti Minimi
(Foot)
1.2 Trigger Points
1.2.1 ABDUCTOR
DIGITI MINIMI (FOOT)
1.3 Organ Reflexes
1.3.1 None
1.3.2 Illustrations
1.4 Meridian
1.4.1 None
1.5 Discussion (Gray)
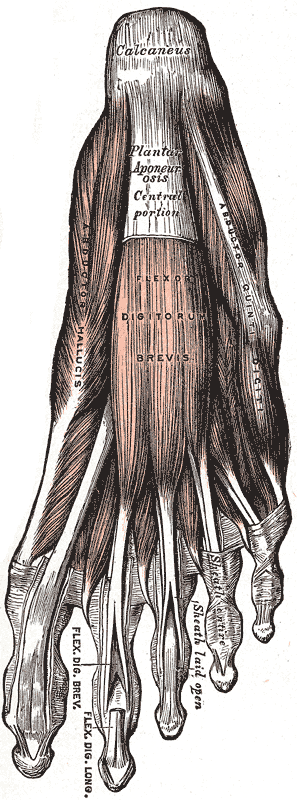
1.5.1 The Abductor digiti quinti (Abductor minimi digiti)
(Fig. 443) Discussion lies along the lateral border
of the foot, and is in relation by its medial margin with the lateral plantar
vessels and nerves. It arises, by a broad origin, from the lateral
process of the tuberosity of the calcaneus, from the under surface of the
calcaneus between the two processes of the tuberosity, from the forepart of the
medial process, from the plantar aponeurosis, and from the intermuscular septum
between it and the Flexor digitorum brevis. Its tendon, after gliding over a
smooth facet on the under surface of the base of the fifth metatarsal bone, is inserted,
with the Flexor digiti quinti brevis, into the fibular side of the base of the
first phalanx of the fifth toe.
1.5.2 Variations —Slips of origin from the tuberosity at the base of the
fifth metatarsal Abductor ossis metatarsi quinti, origin external
tubercle of the calcaneus, insertion into tuberosity of the fifth metatarsal
bone in common with or beneath the outer margin of the plantar fascia
1.5.3 Action-the action of the Abductor digiti quinti is twofold, as an
abductor of this toe from the fourth, and as a flexor of its proximal phalanx.
1.5.4 Non Web Based Links
1.5.4.1 Fig443
(Bitmap)
{kind=link}
1.5.4.2 Discussion
1.5.5 Discussion
1.5.5.1
http://www.bartleby.com/107/131.html
1.5.6 Illustration
1.5.6.1 http://www.bartleby.com/107/illus443.html
1.6 Category
1.6.1 Intrinsic
Foot Plantar First Superficial Layer (IFP1)
1.7 View (When
Illustrated Individually)
1.7.1 Plantar View
(First Plantar Layer)
1.7.2 Test
1.7.2.1
Illus. (DSL) Illus. (Dial-Up)
2 ABDUCTOR DIGITI
MINIMI (HAND)
Back Table of Contents References
2.1 Word Derivation Pronounce
2.1.1 Abductor=Moves
part away from midline
2.1.2 Digit=Finger or
toe
2.1.3 Minimi= Little
finger or toe
2.2 Attachments Illus. (DSL)
2.2.1 Origin
2.2.1.1
Pisiform bone
2.2.1.2
Tendon of the flexor carpi ulnaris
2.2.2 Insertion
2.2.2.1
Two slips
2.2.2.1.1
Ulnar
side of the base of the proximal phalanx of the little finger
2.2.2.1.2
Ulnar
border of the extensor expansion of the finger
2.3 Action Illus. (DSL)
2.3.1 Abducts the little
finger
2.3.2 Assists in flexing
its proximal phalanx at the Metacarpophalangeal joint
2.4 Nerve Supply
2.4.1 Nerve
2.4.1.1
Ulnar (Deep Branch)
2.4.2 Roots
2.4.2.1
C8
2.4.2.2
T1
2.5 Synergists
2.5.1 Flexor digiti
minimi brevis
2.5.2 Opponens digiti
minimi
2.6 Muscle Tests
2.6.1 ABDUCTOR
DIGITI MINIMI (HAND)
2.7 Trigger Points
2.7.1 ABDUCTOR
DIGITI MINIMI (HAND)
2.8 Organ Reflexes
2.8.1 None
2.8.2 Illustrations
2.9 Meridian
2.9.1 None
2.10 Discussion (Gray)
2.10.1
The Abductor digiti
quinti
(Abductor minimi digiti) (Fig. 427) is situated on the ulnar
border of the palm of the hand. It arises from the pisiform bone and
from the tendon of the Flexor carpi ulnaris, and ends in a flat tendon, which
divides into two slips; one is inserted into the ulnar side of the base
of the first phalanx of the little finger; the other into the ulnar border of
the aponeurosis of the Extensor digiti quinti proprius.
2.10.2
Variations
2.10.2.1
The Abductor digiti quinti may be divided into two or three
slips or united with the Flexor digiti quinti brevis.
2.10.3
Actions —The Abductor
digiti quinti abducts the little finger from the ring finger and assist in
flexing the proximal phalanx.
2.10.4
Nerves-C8 Ulnar
2.11 Category
2.11.1
Intrinsic Hand Hypothenar (IHH)
2.12 View (When
Illustrated Individually)
2.12.1
Anterior
2.12.1.1Illus. (DSL)
3 ABDUCTOR HALLUCIS
Back Table of Contents References
3.1 Word Derivation
3.1.1 Abductor=Moves
part away from midline
3.1.2 Hallucis= Hallux
or Great toe
3.2 Attachments Illus. (DSL)
3.2.1 Origin
3.2.1.1
Medial process of tuberosity of the calcaneus
3.2.1.2
Flexor retinaculum
3.2.1.3
Plantar aponeurosis
3.2.1.4
Intermuscular septum
3.3
Insertion
3.3.1.1
Medial tendon of the flexor hallucis
brevis
3.3.1.2
Medial side of the base of the
proximal phalanx of the big toe
3.4 Action Illus. (DSL)
3.4.1 Abducts
the big toe from the mid line of the foot phalangeal
3.5 Nerve Supply
3.5.1 Nerve
3.5.1.1
Medial plantar
3.5.2 Roots
3.5.2.1
L4
3.5.2.2
L5
3.5.2.3
S1
3.5.2.4
S2
3.5.2.5
S3
3.6 Synergists
3.6.1 None
3.7 Muscle Tests
3.7.1 ABDUCTOR HALLUCIS
3.8 Trigger Points
3.8.1 ABDUCTOR
HALLUCIS
3.9 Organ Reflexes
3.9.1 None
3.9.2 Illustrations
3.10 Meridian
3.10.1
None
3.11 Discussion (Gray)
3.11.1
The Abductor hallucis (Fig. 443) lies along the medial border
of the foot and covers the origins of the plantar vessels and nerves. It arises
from the medial process of the tuberosity of the calcaneus, from the laciniate
ligament, from the plantar aponeurosis, and from the intermuscular septum
between it and the Flexor digitorum brevis. The fibers end in a tendon, which
is inserted, together with the medial tendon of the Flexor hallucis
brevis, into the tibial side of the base of the first phalanx of the great toe.
3.11.2
Variations —Slip to the base
of the first phalanx of the second toe.
3.11.3
Action- The Abductor
hallucis abducts the great toe from the second, and also flexes its proximal
phalanx.
3.11.4
Discussion
3.11.4.1http://www.bartleby.com/107/131.html
3.11.5
Illustration
3.11.5.1http://www.bartleby.com/107/illus443.html
3.12 Category
3.12.1
Intrinsic Foot Plantar First Superficial Layer (IFP1)
3.13 View (When
Illustrated Individually)
3.13.1
Plantar View (First Plantar Layer)
3.13.1.1Illus. (DSL)
4 ABDUCTOR POLLICIS
BREVIS B4E4
Back Table of Contents References
4.1 Word Derivation
4.1.1 Abductor=Moves part
away from midline
4.1.2 Pollex= Thumb
4.1.3 Brevis=Short
4.2 Attachments Illus. (DSL)
4.3
Origin
4.3.1.1
Flexor retinaculum
4.3.1.2
Tubercles of the scaphoid and trapezium
4.4
Insertion
4.4.1.1
Radial side of the base of the proximal phalanx of the thumb
4.5 Action Illus. (DSL)
4.5.1 Abduction of the
proximal phalanx and the metacarpal of the thumb
4.5.2 Medial rotation of
the proximal phalanx and the metacarpal of the thumb
4.6 Nerve Supply
4.6.1 Nerve
4.6.1.1
Median
4.6.2 Roots
4.6.2.1
C8
4.6.2.2
T1
4.7 Synergists
4.7.1 Abductor pollicis
longus
4.7.2 Extensor pollicis
brevis
4.8 Muscle Tests
4.8.1 ABDUCTOR
POLLICIS BREVIS
4.9 Trigger Points
4.9.1 ABDUCTOR
POLLICIS BREVIS
4.10 Organ Reflexes
4.10.1
None
4.10.2
Illustrations
4.11 Meridian
4.11.1
None
4.12 Discussion (Gray)
4.12.1
The Abductor pollicis
brevis
(Abductor pollicis) (Fig. 426) (Fig. 427) is a thin, flat muscle, placed
immediately beneath the integument. It arises from the transverse carpal
ligament, the tuberosity of the navicular, and the ridge of the greater
multiangular, frequently by two distinct slips. Running lateralward and
downward, it is inserted by a thin, flat tendon into the radial side of
the base of the first phalanx of the thumb and the capsule of the
metacarpophalangeal articulation.
4.12.2
Variations —The Abductor
pollicis brevis is often divided into an outer and an inner part; accessory
slips from the tendon of the Abductor pollicis longus or Palmaris longus, more
rarely from the Extensor carpi radialis longus, from the styloid process or
Opponens pollicis or from the skin over the thenar eminence.
4.12.3
Actions —The Abductor
pollicis brevis draws the thumb forward in a plane at right angles to that of
the palm of the hand.
4.13 Category
4.13.1
Intrinsic Hand Thenar (ITT)
4.14 View (When
Illustrated Individually)
4.14.1
Anterior View
4.14.1.1Illus. (DSL)
5 ABDUCTOR POLLICIS
LONGUS B5E5
Back Table of Contents References
5.1 Word Derivation
5.1.1 Abductor=Moves
part away from midline
5.1.2 Pollex= Thumb
5.1.3 Longus=Long
5.2 Attachments Illus. 1 (DSL) Illus. 2 (DSL)
5.3
Origin
5.3.1.1
Posterior surface of middle one third of body of radius
5.3.1.2
Posterior lateral surface of the ulna distal to the origin
of the Supinator
5.3.1.3
Interosseous membrane
5.4
Insertion
5.4.1.1
Base of first metacarpal bone, radial side
5.5 Action Illus. (DSL)
5.5.1 Abducts the
carpometacarpal joint of the thumb
5.5.2 Assists in
extension of the carpometacarpal joint of the thumb
5.6 Nerve Supply
5.6.1 Nerve
5.6.1.1
Posterior interosseous nerve (deep radial nerve)
5.6.2 Roots
5.6.2.1
C7
5.6.2.2
C8
5.7 Synergists
5.7.1 Abductor pollicis
brevis
5.7.2 Extensor pollicis
brevis
5.8 Muscle Tests
5.8.1 ABDUCTOR
POLLICIS LONGUS
5.9 Trigger Points
5.9.1 ABDUCTOR
POLLICIS LONGUS
5.10 Organ Reflexes
5.10.1
None
5.10.2
Illustrations
5.11 Meridian
5.11.1
None
5.12 Discussion (Gray)
5.12.1
The Abductor pollicis
longus
(Extensor oss. metacarpi pollicis) (Fig. 419) lies immediately below the
Supinator and is sometimes united with it. It arises from the lateral
part of the dorsal surface of the body of the ulna below the insertion of the
Anconeus, from the interosseous membrane, and from the middle third of the
dorsal surface of the body of the radius. Passing obliquely downward and
lateralward, it ends in a tendon, which runs through a groove on the lateral
side of the lower end of the radius, accompanied by the tendon of the Extensor
pollicis brevis, and is inserted into the radial side of the base of the
first metacarpal bone. It occasionally gives off two slips near its insertion:
one to the greater multiangular bone and the other to blend with the origin of
the Abductor pollicis brevis.
5.12.2
Variations —More or less
doubling of muscle and tendon with insertion of the extra tendon into the first
metacarpal, the greater multiangular, or into the Abductor pollicis brevis or
Opponens pollicis
5.12.3
Action- The chief action
of the Abductor pollicis longus is to carry the thumb laterally from the palm
of the hand. By its continued action, it helps to extend and abduct the wrist.
5.13 Category
5.13.1
Wrist, Hand, and Fingers Posterior Extensors Deep (WHFPED)
5.14 View (When
Illustrated Individually)
5.14.1
Posterior
5.14.1.1Illus. (DSL)
6 ADDUCTOR BREVIS B6E6
Back Table of Contents References
6.1 Word Derivation
6.1.1 Adductor=Moves
part towards the midline
6.1.2 Brevis=Short
6.2 Attachments Illus. 1 (DSL) Illus. 2 (DSL)
6.3
Origin
6.3.1.1
Outer surface of body and inferior ramus of pubis
6.4
Insertion
6.4.1.1
On a line extending from lesser trochanter to upper part of
linea aspera
6.5 Action Illus. (DSL)
6.5.1 Hip adduction
6.5.2 Hip flexion
6.5.3 Hip medial
rotation
6.6 Nerve Supply
6.6.1 Nerve
6.6.1.1
Obturator
6.6.2 Roots
6.6.2.1
L2
6.6.2.2
L3
6.6.2.3
L4
6.7 Synergists
6.7.1 Adductor magnus
6.7.2 Adductor longus
6.7.3 Gracilis
6.7.4 Pectineus
6.8 Muscle Tests
6.8.1 ADDUCTOR
BREVIS
6.9 Trigger Points
6.9.1 ADDUCTOR
BREVIS
6.10 Organ Reflexes
6.10.1
CLIMACTERIC
6.10.2
Illustrations
6.11 Meridian
6.11.1
Pericardium
6.12 Discussion (Gray)
6.12.1
The Adductor brevis (Fig. 433) is situated immediately behind
the two preceding muscles. It is triangular in form, and arises by a narrow
origin from the outer surfaces of the superior and inferior rami of the pubis,
between the Gracilis and Obturator externus. Its fibers, passing backward,
lateralward, and downward, are inserted, by an aponeurosis, into the
line leading from the lesser trochanter to the linea aspera and into the upper
part of the linea aspera, immediately behind the Pectineus and upper part of
the Adductor longus
6.12.2
Variations- the Adductor brevis may be divided into
two or three parts, or it may be united to the Adductor magnus.
6.12.3
Action- the Pectineus and three Adductores adduct the thigh
powerfully; they are especially used in horse exercise, the sides of the saddle
being grasped between the knees by the contraction of these muscles. In
consequence of the obliquity of their insertions into the linea aspera, they
rotate the thigh outward, assisting the external Rotators, and when the limb
has been abducted, they draw it medialward, carrying the thigh across that of
the opposite side. The Pectineus and Adductores brevis and longus assist the
Psoas major and Iliacus in flexing the thigh upon the pelvis. In progression,
all these muscles assist in drawing forward the lower limb.
6.13 Category
6.13.1
Thigh Adductor Compartment (TAD)
6.14 View (When Illustrated
Individually)
6.14.1
Anterior
6.14.1.1Illus. (DSL)
7 ADDUCTOR HALLUCIS B7E7
Back Table of Contents References
7.1 Word Derivation
7.1.1 Adductor=Moves
part towards the midline
7.1.2 Hallucis= Hallux
or Great toe
7.2 Attachments Illus. (DSL)
7.2.1 Origin
7.2.1.1
Oblique head
7.2.1.1.1
Bases
of the 2nd, 3rd and
4th metatarsals
7.2.1.1.2
Sheath
of tendon of Peroneus Longus
7.2.1.2
Transverse head
7.2.1.2.1
Plantar
Metatarsophalangeal ligaments of the 3rd, 4th and 5th toes
7.2.1.2.2
Deep
transverse metatarsal ligaments
7.2.2 Insertion
7.2.2.1
Lateral side of base of proximal phalanx of big toe
7.3 Action Illus. (DSL)
7.3.1 Adduction
(big toe towards the 2nd toe)
7.3.2 Flexion
(big toe towards plantar surface)
7.4 Joints
7.4.1 Metatarsophalangeal
joint of big toe
7.5 Nerve Supply
7.5.1 Nerve
7.5.1.1
Lateral plantar nerve
7.5.2 Roots
7.5.2.1
S2
7.5.2.2
S3
7.6 Synergists
7.6.1
7.7 Muscle Tests
7.7.1 ADDUCTOR
HALLUCIS
7.8 Trigger Points
7.8.1 ADDUCTOR
HALLUCIS
7.9 Organ Reflexes
7.9.1 None
7.9.2 Illustrations
7.10 Meridian
7.10.1
None
7.11 Discussion (Grays)
7.11.1
The Adductor hallucis (Adductor obliquus
hallucis) (Fig. 445) arises
by two heads—oblique and transverse. The oblique
head
is a large, thick, fleshy mass, crossing the foot obliquely and occupying the
hollow space under the first second, third, and fourth metatarsal bones. It arises
from the bases of the second, third, and fourth metatarsal bones, and from the
sheath of the tendon of the Peroneus longus, and is inserted, together
with the lateral portion of the Flexor hallucis brevis, into the lateral side
of the base of the first phalanx of the great toe. The transverse head (Transversus pedis) is a narrow, flat fasciculus
which arises from the plantar metatarsophalangeal ligaments of the
third, fourth, and fifth toes (sometimes only from the third and fourth), and
from the transverse ligament of the metatarsus. It is inserted into the
lateral side of the base of the first phalanx of the great toe, its fibers
blending with the tendon of insertion of the oblique head.
7.11.2
Variations
7.11.2.1
Slips to the base of the first phalanx of the second toe Opponens
hallucis, occasional slips from the adductor to the metatarsal bone of the
great toe
7.11.2.2
The Abductor, Flexor brevis, and Adductor of the great toe,
like the similar muscles of the thumb, give off, at their insertions, fibrous
expansions to blend with the tendons of the Extensor digitorum longus.
7.11.3
Action- the Abductor hallucis abducts the great toe from the
second, and flexes its proximal phalanx.
7.11.4
Discussion
7.11.4.1http://www.bartleby.com/107/131.html
7.11.5
Illustration
7.11.5.1http://www.bartleby.com/107/illus445.html
7.12 Category
7.12.1
Intrinsic Foot Plantar Third Layer (IFP3)
7.13 View (When
Illustrated Individually)
7.13.1
Plantar
7.13.1.1.1
Illus. (DSL)
8 ADDUCTOR LONGUS B8E8
Back Table of Contents References
8.1 Word Derivation
8.1.1 Adductor=Moves
part towards the midline
8.1.2 Longus=Long
8.2 Attachments Illus. 1 (DSL) Illus. 2 (DSL)
8.2.1 Origin
8.2.1.1
Anterior pubis in angle between crest and symphysis
8.2.2 Insertion
8.2.2.1
Middle 1/3 of medial lip of linea
aspera
8.3 Joints
8.3.1 Hip
8.4 Action Illus. (DSL)
8.4.1 Adduction
8.4.2 Flexion
8.4.3 Medial
rotation
8.5 Nerve Supply
8.5.1 Nerve
8.5.1.1
Obturator
8.5.2 Roots
8.5.2.1
L2
8.5.2.2
L3
8.5.2.3
L4
8.6 Synergists
8.6.1 Gracilis
8.6.2 Adductor
magnus
8.6.3 Pectineus
8.6.4 Adductor
brevis
8.7 Muscle Tests
8.7.1 ADDUCTOR
LONGUS
8.8 Trigger Points
8.8.1 ADDUCTOR
LONGUS
8.9 Organ Reflexes
8.9.1 CLIMACTERIC
8.9.2 Illustrations
8.10 Meridian
8.10.1
Pericardium
8.11 Discussion (Gray)
8.11.1
The Adductor longus (Fig 432) (Fig. 433), the most superficial
of the three Adductores, is a triangular muscle, lying in the same plane as the
Pectineus. It arises by a flat, narrow tendon, from the front of the
pubis, at the angle of junction of the crest with the symphysis; and soon
expands into a broad fleshy belly. This passes downward, backward, and
lateralward, and is inserted, by an aponeurosis, into the linea aspera,
between the Vastus medialis and the Adductor magnus, with both of which it is
usually blended.
8.11.2
Variations-The Adductor longus may be double, may
extend to the knee, or be more or less united with the Pectineus.
8.11.3
Action-The Pectineus and three Adductores adduct the thigh
powerfully; they are especially used in horse exercise, the sides of the saddle
being grasped between the knees by the contraction of these muscles. In
consequence of the obliquity of their insertions into the linea aspera, they
rotate the thigh outward, assisting the external Rotators, and when the limb
has been abducted, they draw it medialward, carrying the thigh across that of
the opposite side. The Pectineus and Adductores brevis and longus assist the
Psoas major and Iliacus in flexing the thigh upon the pelvis. In progression,
all these muscles assist in drawing forward the lower limb.
8.12 Category
8.12.1
Thigh Adductor Compartment (TAD)
8.13 View (When
Illustrated Individually)
8.13.1
Anterior
8.13.1.1Illus. (DSL)
9 ADDUCTOR MAGNUS B9E9
Back Table of Contents References
9.1 Word Derivation
9.1.1 Adductor=Moves
part towards the midline
9.1.2 Magnus=Large
9.2 Attachments Illus. 1 (DSL) Illus. 2 (DSL)
9.2.1 Origin
9.2.1.1
POSTERIOR FIBERS
9.2.1.1.1
Ischial
tuberosity
9.2.1.2
ANTERIOR FIBERS
9.2.1.2.1
Ramus
of ischium
9.2.1.2.2
Inferior
pubic ramus
9.2.2 Insertion
9.2.2.1
Line extending from the greater
trochanter along the linea aspera
9.2.2.2
Medial supracondylar line
9.2.2.3
Adductor tubercle on medial condyle
of femur
9.3 Joints
9.3.1 Hip
9.4 Action Illus. (DSL)
9.4.1 Adduction
9.4.2 Extension
9.4.2.1
. Note
9.4.2.1.1
Fibers arising from ischium and ramus of ischium primarily
insert distally and aid in hip extension
9.4.3 Flexion
9.4.3.1
Note
9.4.3.1.1 Fibers
arising from ramus of pubis insert proximally and aid in hip flexion.
9.4.4 Medial
rotation
9.5 Nerve Supply
9.5.1 Posterior
fibers
9.5.1.1
Nerve
9.5.1.1.1 Tibial
portion of sciatic
9.5.1.2
Roots
9.5.1.2.1 L4
9.5.1.2.2 L5
9.5.1.2.3 S1
9.5.2 Anterior
fibers
9.5.2.1
Nerve
9.5.2.1.1 Obturator
9.5.2.2
Roots
9.5.2.2.1 L2
9.5.2.2.2 L3
9.5.2.2.3 L4
9.6 Synergists
9.6.1 Adductor
brevis
9.6.2 Adductor
longus
9.6.3 Pectineus
9.6.4 Gracilis
9.7 Muscle Tests
9.7.1 ADDUCTOR
MAGNUS
9.8 Trigger Points
9.8.1 ADDUCTOR
MAGNUS
9.9 Organ Reflexes
9.9.1 CLIMACTERIC
9.9.2 Illustrations
9.10 Meridian
9.10.1
Pericardium
9.11 Discussion (Gray)
9.11.1
The Adductor magnus Fig 432 (Fig. 433) is a large triangular muscle, situated on the
medial side of the thigh. It arises from a small part of the inferior
ramus of the pubis, from the inferior ramus of the ischium, and from the outer
margin of the inferior part of the tuberosity of the ischium. Those fibers
which arise from the ramus of the pubis are short, horizontal in direction, and
are inserted into the rough line leading from the greater trochanter to the
linea aspera, medial to the Glutæus maximus; those from the ramus of the
ischium are directed downward and lateralward with different degrees of
obliquity, to be inserted, by means of a broad aponeurosis, into the
linea aspera and the upper part of its medial prolongation below. The medial
portion of the muscle, composed principally of the fibers arising from the
tuberosity of the ischium, forms a thick fleshy mass consisting of coarse
bundles which descend almost vertically, and end about the lower third of the
thigh in a rounded tendon which is inserted into the adductor tubercle on the
medial condyle of the femur, and is connected by a fibrous expansion to the
line leading upward from the tubercle to the linea aspera. At the insertion
of the muscle, there is a series of osseoaponeurotic openings, formed by
tendinous arches attached to the bone. The upper four openings are small, and
give passage to the perforating branches of the profunda femoris artery. The
lowest is of large size, and transmits the femoral vessels to the popliteal fossa.
9.11.2
Variations-The Adductor magnus may be more or less
segmented; the anterior and superior portion is often described as a separate
muscle, the Adductor minimus. The muscle may be fused with the Quadratus
femoris.
9.11.3
Action-The Pectineus and three Adductores adduct the thigh
powerfully; they are especially used in horse exercise, the sides of the saddle
being grasped between the knees by the contraction of these muscles. In
consequence of the obliquity of their insertions into the linea aspera, they
rotate the thigh outward, assisting the external Rotators, and when the limb
has been abducted, they draw it medialward, carrying the thigh across that of
the opposite side.
9.12 Category
9.12.1
Thigh Adductor Compartment (TAD)
9.13 View (When
Illustrated Individually)
9.13.1
Anterior
9.13.1.1Illus. (DSL)
10 ADDUCTOR POLLICIS B10E10
Back Table of Contents References
10.1 Word Derivation
10.1.1
Adductor=Moves part towards the midline
10.1.2
Pollex= Thumb
10.2 Attachments Illus. (DSL)
10.2.1
Origin
10.2.1.1OBLIQUE HEAD
10.2.1.1.1
Capitate
bone
10.2.1.1.2
Bases
of the 2nd and 3rd metacarpal bones
10.2.1.1.3
Intercarpal
ligaments
10.2.1.1.4
Sheath
of the tendon of the Flexor carpi radialis
10.2.1.2TRANSVERSE HEAD
10.2.1.2.1
Distal
2/3 of the palmar surface of the 3rd metacarpal bone
10.2.2
Insertion
10.2.2.1Two heads
converge to insert on the ulnar side of the base of the proximal phalanx of the
thumb
10.3 Joints
10.3.1
Carpometacarpal (CMJ)
10.3.2
Metacarpophalangeal (MPJ)
10.4 Action Illus. (DSL)
10.4.1
Adduction (1st CMJ)
(Thumb)
10.4.2
Adduction (1st MPJ)
(Thumb)
10.4.3
Flexion (1st MPJ) (Thumb)
10.5 Nerve Supply
10.5.1
Nerve
10.5.1.1
Ulnar (Deep branch)
10.5.2
Roots
10.5.2.1
C8
10.5.2.2
T1
10.6 Synergists
10.6.1
Flexor pollicis brevis
10.6.2
Flexor pollicis longus
10.6.3
Opponens pollicis
10.7 Muscle Tests
10.7.1
ADDUCTOR POLLICIS
10.8 Trigger Points
10.8.1
ADDUCTOR POLLICIS
10.9 Organ Reflexes
10.9.1
None
10.9.2
Illustrations
10.10
Meridian
10.10.1
None
10.11
Discussion (Gray)
10.11.1
The Adductor pollicis (obliquus) (Adductor obliquus pollicis) (Fig. 426) arises by several slips from the capitate
bone, the bases of the second and third metacarpals, the intercarpal ligaments,
and the sheath of the tendon of the Flexor carpi radialis. From this origin the
greater number of fibers pass obliquely downward and converge to a tendon,
which, uniting with the tendons of the medial portion of the Flexor pollicis
brevis and the transverse part of the Adductor, is inserted into the
ulnar side of the base of the first phalanx of the thumb, a sesamoid bone being
present in the tendon. A considerable fasciculus, however, passes more
obliquely beneath the tendon of the Flexor pollicis longus to join the lateral
portion of the Flexor brevis and the Abductor pollicis brevis.
10.11.2
The Adductor pollicis (transversus) (Adductor transversus pollicis) (Fig. 426) Fig 427 is the most deeply seated of this group of muscles.
It is of a triangular form arising by a broad base from the lower two-thirds of
the volar surface of the third metacarpal bone; the fibers converge, to be inserted
with the medial part of the Flexor pollicis brevis and the Adductor pollicis
(obliquus) into the ulnar side of the base of the first phalanx of the thumb
10.11.3
Variations-The two adductors
vary in their relative extent and in the closeness of their connection. The
Adductor obliquus may receive a slip from the transverse metacarpal ligament.
10.11.4
Actions-The Abductor
pollicis brevis draws the thumb forward in a plane at right angles to that of
the palm of the hand. The Adductor pollicis is the opponent of this muscle, and
approximates the thumb to the palm.
10.12
Category
10.12.1
Intrinsic Hand Thenar (IHT)
10.13
View (When Illustrated Individually)
10.13.1
Anterior
10.13.1.1 Illus. (DSL)
11 ANCONEUS B11E11
Back Table of Contents References
11.1 Word Derivation
11.1.1
Anconeal=Pertaining to elbow
11.2 Attachments Illus.1
(DSL) Illus.2
(DSL)
11.2.1
Origin
11.2.1.1Posterior surface of lateral
Epicondyle of humerus
11.2.2
Insertion
11.2.2.1Lateral
side of Olecranon process
11.2.2.2Upper
1/4th of posterior surface of proximal portion of ulna
11.3 Joints
11.3.1
Elbow
11.3.2
Radioulnar (RU)
11.4 Action Illus. (DSL)
11.4.1
Extension (Elbow)
11.4.2
Pronation (RU)
11.5 Nerve Supply
11.5.1
Nerve
11.5.1.1
Radial
11.5.2
Roots
11.5.2.1
C7
11.5.2.2
C8
11.5.2.3
T1
11.6 Synergists
11.6.1
Triceps Brachii
11.7 Muscle Tests
11.7.1
ANCONEUS
11.8 Trigger Points
11.8.1
ANCONEUS
11.9 Organ Reflexes
11.9.1
Pancreas
11.9.2
Illustrations
11.10
Meridian
11.10.1 Spleen/Pancreas
11.11
Discussion (Gray)
11.11.1
The Anconæus (Fig. 418) is a small triangular muscle, which is placed on the back
of the elbow-joint, and appears to be a continuation of the Triceps brachii. It
arises by a separate tendon from the back part of the lateral epicondyle
of the humerus; its fibers diverge and are inserted into the side of the
olecranon, and upper fourth of the dorsal surface of the body of the ulna.
11.11.2
Actions-The Anconæus assists the Triceps in extending the
forearm.
11.12
Category
11.12.1
Forearm Extensors (FAE)
11.13
View (When Illustrated Individually)
11.13.1
Posterior
11.13.1.1 Illus. (DSL)
12 BICEPS BRACHII B12E12
Back Table of Contents References
12.1 Word Derivation
and Pronunciation
12.2
Pronunciation
12.2.1.1BICEPS BRA·CHII- 'bI-"seps 'brA-kE-"I, -kE-"E 
12.2.1.2Pronunciation Key
12.2.1
Etymology
12.2.1.1Biceps=Two heads of origin
12.2.1.1.1
New
Latin bicipit-, biceps, from Latin, two-headed, from bi- + capit-,
caput head
12.2.1.2Brachion=Upper Arm
12.1 Attachments Illus. 1 Illus. 2
12.1.1
Origin
12.1.1.1Long head
12.1.1.1.1
Supraglenoid
tubercle of the scapula
12.1.1.2Short head
12.1.1.2.1
Apex
of coracoid process of the scapula
12.1.2
Insertion
12.1.2.1Radial
tuberosity
12.1.2.2Bicipital
aponeurosis (lacertus fibrosus) (Continuous with the
deep fascia covering the origins of the Flexor muscles)
12.2 Joints
12.2.1
Glenohumeral (GH)
12.2.2
Elbow
12.2.3
Radioulnar (RU)
12.3 Action Video
12.3.1
Flexion (Elbow)
12.3.2
Supination (RU)
12.3.3
Flexion (GH)
12.3.4
Reversed origin-insertion action
12.3.4.1
Both heads of the biceps brachii are active during flexion
of the arm at the shoulder joint, with the long head being more active.
12.4 Nerve Supply
12.4.1
Nerve
12.4.1.1
Musculocutaneous
12.4.1.1.1
Separate branches to each head
12.4.2
Roots
12.4.2.1
C5
12.4.2.2
C6
12.5 Synergists
12.5.1
Brachialis
12.5.2
Brachioradialis
12.5.3
Supinator
12.1 Muscle Tests
12.1.1
BICEPS BRACHII
12.2 Trigger Points
12.2.1
BICEPS BRACHII
12.3 Organ Reflexes
12.3.1
Stomach
12.3.2
Illustrations
12.4 Acupressure/Acupuncture
Theory
12.4.1
Organs
12.4.1.1Spleen/Stomach
12.4.2
Channels Discussion
12.4.2.1Spleen/Stomach
12.4.3
Channels Illustration All
12.4.3.1Stomach ALL
12.4.4
Channels Illus Command Points
12.4.4.1Stomach
12.5 Musculoskeletal
Pathology
12.5.1
BICEPS TENDINTIS
(Proximal)
12.5.2
BICEPS TENDINTIS (Distal)
12.6 Orthopaedic Tests
12.6.1
Biceps Strength
12.6.2
Bicipital Tendinitis Test
12.6.3
Impingement Syndrome Test
12.6.4
Reflexes (Shoulder)
12.6.5
Yergason's Test
12.7 Musculoskeletal
Examination
12.7.1
Shoulder and Shoulder Girdle
12.7.2
Elbow
12.8 Stretching
12.8.1
Stretching
Concepts
12.8.2
Stretching
Individual Muscle Discussion
12.8.3
Stretching
Muscle Illustration
12.9 Posture
12.9.1
Postural
Assessment
12.9.2
Postural
Illustrations
12.10 Massage Routines
12.10.1
Deep Tissue
12.10.1.1 Deltoid
12.10.1.2 Biceps
Triceps
12.11
Exercise
12.11.1
Biceps Brachii-Resistance Exercise
12.11.2
Biceps Brachii- Biomechanics
12.12
Discussion (Gray)
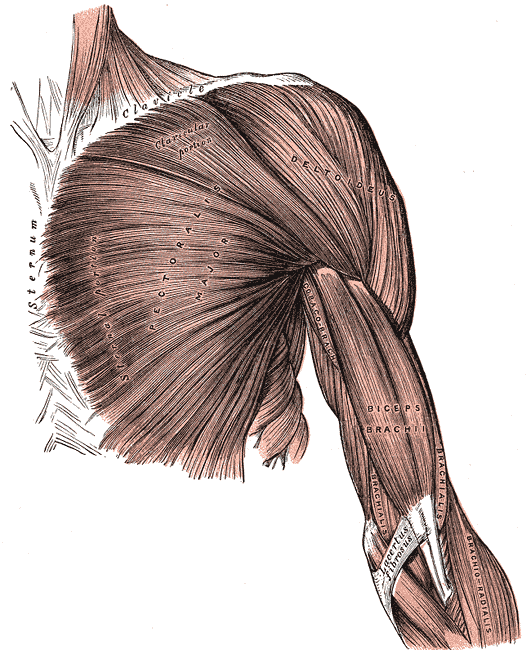
12.12.1
The Biceps brachii (Biceps;
Biceps flexor cubiti) (Fig. 411) Discussion is a long fusiform muscle,
placed on the front of the arm, and arising by two heads, from which
circumstance it has received its name. The short
head
arises by a thick flattened tendon from the apex of the coracoid
process, in common with the Coracobrachialis. The long
head
arises from the supraglenoid tuberosity at the upper margin of the
glenoid cavity, and is continuous with the glenoidal labrum. This tendon,
enclosed in a special sheath of the synovial membrane of the shoulder-joint,
arches over the head of the humerus; it emerges from the capsule through an
opening close to the humeral attachment of the ligament, and descends in the
intertubercular groove; it is retained in the groove by the transverse humeral
ligament and by a fibrous prolongation from the tendon of the Pectoralis major.
An elongated muscular belly succeeds each tendon, and the two bellies, although
closely applied to each other, can readily be separated until within about 7.5
cm. of the elbow-joint. Here they end in a flattened tendon, which is inserted
into the rough posterior portion of the tuberosity of the radius, a bursa being
interposed between the tendon and the front part of the tuberosity. As the
tendon of the muscle approaches the radius it is twisted upon itself, so that
its anterior surface becomes lateral and is applied to the tuberosity of the
radius at its insertion. Opposite the bend of the elbow the tendon gives off,
from its medial side, a broad aponeurosis, the lacertus
fibrosus
(bicipital fascia) which passes obliquely downward and medialward across
the brachial artery, and is continuous with the deep fascia covering the
origins of the Flexor muscles of the forearm (Fig. 410).
12.12.2
Variations —A third head (10
per cent.) to the Biceps brachii is occasionally found, arising at the upper
and medial part of the Brachialis, with the fibers of which it is continuous, and
inserted into the lacertus fibrosus and medial side of the tendon of the
muscle. In most cases, this additional slip lies behind the brachial artery in
its coarse down the arm. In some instances, the third head consists of two
slips, which pass down, one in front of and the other behind the artery,
concealing the vessel in the lower half of the arm. More rarely a fourth head
occurs arising from the outer side of the humerus, from the intertubercular
groove, or from the greater tubercle. Other heads are occasionally found. Slips
sometimes pass from the inner border of the muscle over the brachial artery to
the medial intermuscular septum or the medial epicondyle or more rarely to the
Pronator teres or Brachialis. The long head may be absent or arise from the
intertubercular groove.
12.12.3
Actions- The Biceps
brachii is a flexor of the elbow and, to a less extent, of the shoulder; it is
also a powerful Supinator, and serves to render tense the deep fascia of the
forearm by means of the lacertus fibrosus given off from its tendon.
12.12.4
Non Web Based
Links
12.12.4.1 Fig. 410
{kind=link}
12.12.4.2 Fig. 411
{kind=link}
12.12.4.3 Discussion
12.13
Quiz
12.13.1
Test Your Knowledge
12.14
Category
12.14.1
Forearm Flexors (FAF)
12.15
View (When Illustrated Individually)
12.15.1
Anterior
12.15.1.1 Illus. (DSL)
1 BICEPS
FEMORIS (Lateral Hamstring) B13E13
Back Table of Contents References
1.1 Word Derivation
1.1.1 Biceps=Two heads
of origin
1.1.2 Femoris=Femur
1.2 Attachments Illus. (DSL)
1.2.1 Origin
1.2.1.1
Long head
1.2.1.1.1
Ischial
tuberosity (Posterior Lower & Inner Impression)
1.2.1.1.2
Sacrotuberous
ligament
1.2.1.2
Short head
1.2.1.2.1
Lateral
lip of linea aspera
1.2.1.2.2
Proximal
2/3rd of lateral supracondylar line of femur
1.2.1.3 Lateral
intermuscular septum
1.2.2 Insertion
1.2.2.1
Lateral side of the head of the fibula
1.2.2.2
Lateral condyle of the tibia
1.2.2.3
Deep fascia on the lateral side of
the leg
1.3 Joints
1.3.1 Knee
1.3.2 Hip
1.4 Action Illus. (DSL)
1.4.1 Long and Short
Head
1.4.1.1
Flexion (Knee)
1.4.1.2
Lateral rotation (Knee)
1.4.2 Long Head Only
1.4.2.1
Extension (Hip)
1.4.2.2
Adduction (Hip)
1.4.2.3
Lateral Rotation (Hip)
1.4.2.4
Note
1.4.2.4.1
When
the hip is extended the long head of the biceps Femoris is placed at a
mechanical disadvantage in knee extension. The short head of the biceps Femoris
then becomes the primary knee flexor.
1.4.2.5
Reversed origin-insertion action
1.4.2.5.1
The
long head gives posterior stability to the pelvis and extends the pelvis on the
hip.
1.5 Nerve Supply
1.5.1 LONG
HEAD
1.5.1.1
Nerve
1.5.1.1.1
Sciatic (Tibial Portion)
1.5.1.2
Roots
1.5.1.2.1
L5
1.5.1.2.2
S1
1.5.1.2.3 S2
1.5.2 Short
head
1.5.2.1 Nerve
1.5.2.1.1 Sciatic
(Common peroneal portion)
1.5.2.2
Roots
1.5.2.2.1 L5
1.5.2.2.2 S1
1.5.2.2.3 S2
1.6 Synergists
1.6.1 Semimembranosus
1.6.2 Semitendinosus
1.6.3 Gracilis
1.6.4 Sartorius
1.6.5 Gastrocnemius
1.7 Muscle Tests
1.7.1 BICEPS
FEMORIS
1.8 Trigger Points
1.8.1 BICEPS FEMORIS
1.9 Organ Reflexes
1.9.1 Rectum
1.9.2 Illustrations
1.10 Meridian
1.10.1
Large Intestine
1.11 Discussion (Gray)
1.11.1
The Biceps femoris (Biceps) (Fig. 434) is situated on the posterior and lateral aspect
of the thigh. It has two heads of origin; one, the long
head,
arises from the lower and inner impression on the back part of the
tuberosity of the ischium, by a tendon common to it and the Semitendinosus, and
from the lower part of the sacrotuberous ligament; the other, the short head, arises from the lateral lip of the linea aspera,
between the Adductor magnus and Vastus lateralis, extending up almost as high
as the insertion of the Gluteus maximus; from the lateral prolongation of the
linea aspera to within 5 cm. of the lateral condyle; and from the lateral
intermuscular septum. The fibers of the long head form a fusiform belly, which
passes obliquely downward and lateralward across the sciatic nerve to end in an
aponeurosis which covers the posterior surface of the muscle, and receives the
fibers of the short head; this aponeurosis becomes gradually contracted into a
tendon, which is inserted into the lateral side of the head of the
fibula, and by a small slip into the lateral condyle of the tibia. At its
insertion, the tendon divides into two portions, which embrace the fibular
collateral ligament of the knee-joint. From the posterior border of the tendon,
a thin expansion is given off to the fascia of the leg. The tendon of insertion
of this muscle forms the lateral hamstring; the common peroneal nerve descends
along its medial border
1.11.2
Variations —The short head
may be absent; additional heads may arise from the ischial tuberosity, the
linea aspera, and the medial supracondylar ridge of the femur or from various
other parts. A slip may pass to the Gastrocnemius.
1.11.3
Actions —The hamstring
muscles flex the leg upon the thigh. When the knee is semiflexed, the Biceps
femoris in consequence of its oblique direction rotates the leg outward; and
the Semitendinosus, and to a slight extent the Semimembranosus, rotate the leg
inward, assisting the Popliteus. Taking their fixed point from below, these
muscles serve to support the pelvis upon the head of the femur, and to draw the
trunk directly backward, as in raising it from the stooping position or in
feats of strength, when the body is thrown backward in the form of an arch. As
already indicated on page 285, complete flexion of the hip cannot be affected
unless the knee-joint is also flexed, because of the shortness of the hamstring
muscles.
1.12 Category
1.12.1
Leg Posterior Flexor Compartment (LPF)
1.13 View (When
Illustrated Individually)
1.13.1
Posterior
1.13.1.1Illus. (DSL)
2 BRACHIALIS B14E14
Back Table of Contents References
2.1 Word Derivation
2.1.1 Brachion=Arm
2.2 Attachments Illus. 1
(DSL) Illus. 2
(DSL)
2.2.1 Origin
2.2.1.1
Deltoid tuberosity (embraces by two
angular processes)
2.2.1.2
Humerus (Lower ½) (Anterior) (To
within 2.5 cm of articular margin)
2.2.1.3
Intermuscular Septa (More Medial than Lateral)
2.2.2 Insertion
2.2.2.1
Tuberosity of the ulna
2.2.2.2
Coronoid process of the ulna (Rough depression on
the anterior surface)
2.3 Joints
2.3.1 Elbow
2.4 Action Illus. (DSL)
2.4.1 Flexion
2.5 Nerve Supply
2.5.1 Nerve
2.5.1.1
Musculocutaneous
2.5.1.2 Radial
2.5.2 Roots
2.5.2.1 C5
(Musculocutaneous)
2.5.2.2 C6
(Musculocutaneous)
2.5.2.3
C7 (Radial)
2.6 Synergists
2.6.1 Brachioradialis
2.6.2 Biceps
brachii
2.7 Muscle Tests
2.7.1 BRACHIALIS
2.8 Trigger Points
2.8.1 BRACHIALIS
2.9 Organ Reflexes
2.9.1 Stomach
2.9.2 Illustrations
2.10 Meridian
2.10.1
Stomach
2.11 Discussion (Gray)
2.11.1
The Brachialis (Brachialis
anticus) (Fig. 411) covers the front of the
elbow-joint and the lower half of the humerus. It arises from the lower
half of the front of the humerus, commencing above at the insertion of the
Deltoideus, which it embraces by two angular processes. Its origin extends
below to within 2.5 cm. of the margin of the articular surface. It also arises
from the intermuscular septa, but more extensively from the medial than the
lateral; it is separated from the lateral below by the Brachioradialis and
Extensor carpi radialis longus. Its fibers converge to a thick tendon, which is
inserted into the tuberosity of the ulna and the rough depression on the
anterior surface of the coronoid process.
2.11.2
Variations —Occasionally
doubled; additional slips to the Supinator, Pronator teres, Biceps, lacertus
fibrosus, or radius are more rarely found.
2.11.3
Actions- the Brachialis is a flexor of the forearm, and
forms an important defence to the elbow-joint. When the forearm is fixed, the
Biceps brachii and Brachialis flex the arm upon the forearm, as in efforts of
climbing.
2.12 Category
2.12.1
Forearm Flexors (FAF)
2.13 View
2.13.1
Anterior
2.13.1.1Illus. (DSL)
3 BRACHIORADIALIS B15E15
Back Table of Contents References
3.1 Word Derivation
3.1.1 Brachion=Arm
3.1.2 Radialis=Radius
3.2 Attachments Illus.1
(DSL) Illus.2
(DSL)
3.2.1 Origin
3.2.1.1
Humerus (Lateral supracondylar
ridge) (Proximal 2/3)
3.2.1.2
Intermuscular septum (Lateral)
3.2.2 Insertion
3.2.2.1
Radius (Styloid Process-Base-Lateral
Side)
3.3 Joints
3.3.1 Elbow
3.3.2 Radioulnar (RU)
Distal
3.4 Action Illus. (DSL)
3.4.1 Flexion
3.4.2 Pronation
(To midposition when joint is supinated) (RU) Distal
3.4.3 Supination
(To midposition when joint is Pronated) (RU) Distal
3.5 Nerve Supply
3.5.1 Nerve
3.5.1.1
Radial
3.5.2 Roots
3.5.2.1
C5
3.5.2.2
C6
3.5.2.3
C7
3.6 Synergists
3.6.1 Brachialis
3.6.2 Biceps
brachii
3.7 Muscle Tests
3.7.1 BRACHIORADIALIS
3.8 Trigger Points
3.8.1 BRACHIORADIALIS
3.9 Organ Reflexes
3.9.1 Stomach
3.9.2 Illustrations
3.10 Meridian
3.10.1
Stomach
3.11 Discussion (Gray)
3.11.1
The Brachioradialis (Supinator
longus) (Fig. 414) (Fig. 417) (Fig. 418) is the most superficial
muscle on the radial side of the forearm. It arises from the upper
two-thirds of the lateral supracondylar ridge of the humerus, and from the
lateral intermuscular septum, being limited above by the groove for the radial
nerve. Interposed between it and the Brachialis are the radial nerve and the
anastomosis between the anterior branch of the profunda artery and the radial
recurrent. The fibers end above the middle of the forearm in a flat tendon,
which is inserted into the lateral side of the base of the styloid
process of the radius. The tendon is crossed near its insertion by the tendons
of the Abductor pollicis longus and Extensor pollicis brevis; on its ulnar,
side is the radial artery.
3.11.2
Variations —Fusion with the
Brachialis; tendon of insertion may be divided into two or three slips;
insertion partial or complete into the middle of the radius, fasciculi to the
tendon of the Biceps, the tuberosity or oblique line of the radius; slips to
the Extensor carpi radialis longus or Abductor pollicis longus; absence; rarely
doubled.
3.11.3
Actions-The
Brachioradialis is a flexor of the elbow-joint, but only acts as such when the
Biceps brachii and Brachialis have initiated the movement of flexion.
3.12 Category
3.12.1
Forearm Flexors (FAF)
3.13 View
3.13.1
Anterior
3.13.1.1Illus. (DSL)
4 BUCCINATOR B16E16
Back Table of Contents References
4.1 Word Derivation
4.1.1 Bucc=Cheek
4.1.2 Buccina=a trumpet
4.2 Attachments
4.2.1 Origin
4.2.1.1
Upper attachment
4.2.1.1.1
Maxilla
(External surfaces of the alveolar process) (Corresponding to the three molar
teeth) (Crossing the maxillary tuberosity to the pterygold hamulus)
4.2.1.2
Middle attachment
4.2.1.2.1
Pterygomandibular
raphe (Anterior border)
4.2.1.3
Inferior attachment
4.2.1.3.1
Mandible
(External surfaces of the alveolar processes) (Corresponding to the three molar
teeth) (Crossing the junction of the ramus and body to the posterior end of the
mylohyoid line)
4.2.1.3.2
Mandible
(Buccinator Ridge)
4.2.2 Insertion
4.2.2.1
Upper fibers
4.2.2.1.1
Orbicularis
Oris (Blend with upper fibers)
4.2.2.2
Middle fibers
4.2.2.2.1
Orbicularis
Oris (Decussate (cross) so that lower and upper ones continue into upper and
lower parts of the Orbicularis Oris)
4.2.2.3
Lower fibers
4.2.2.3.1
Blend
with lower fibers of orbicularis oris
4.3 Action Illus. (DSL)
4.3.1 Compresses
the cheeks against the teeth
4.3.2 Draws
angle of the mouth laterally.
4.4 Nerve Supply
4.4.1 Facial
(VII)
4.4.2 Inferior
buccal branch
4.5 Arterial supply
4.5.1 Buccal
(Maxillary)
4.5.2 Facial
4.5.3 Transverse
facial
4.6 Synergists
4.6.1 Risorius
4.7 Antagonists
4.7.1 Orbicularis
oris
4.8 Muscle Tests
4.8.1 BUCCINATOR
4.9 Trigger Points
4.9.1 BUCCINATOR
4.10 Organ Reflexes
4.10.1
None
4.10.2
Illustrations
4.11 Meridian
4.11.1
None
4.12 Discussion (Gray)
4.12.1
The Buccinator (Fig. 380) (Fig. 381) is a thin quadrilateral muscle, occupying the
interval between the maxilla and the mandible at the side of the face. It arises
from the outer surfaces of the alveolar processes of the maxilla and mandible,
corresponding to the three molar teeth; and behind, from the anterior border of
the pterygomandibular raphé which separates it from the Constrictor pharyngis
superior. The fibers converge toward the angle of the mouth, where the central
fibers intersect each other, those from below being continuous with the upper
segment of the Orbicularis oris, and those from above with the lower segment;
the upper and lower fibers are continued forward into the corresponding lip
without decussation.
4.12.2
Relations —The Buccinator
is covered by the buccopharyngeal fascia, and is in relation by its superficial
surface, behind, with a large mass of fat, which separates it from the
ramus of the mandible, the Masseter, and a small portion of the Temporalis;
this fat has been named the suctorial pad, because it is supposed to
assist in the act of sucking. The parotid duct pierces the Buccinator opposite
the second molar tooth of the maxilla. The deep surface is in relation
with the buccal glands and mucous membrane of the mouth.
4.12.3
Actions- The Buccinators
compress the cheeks, so that, during the process of mastication, the food is
kept under the immediate pressure of the teeth. When the cheeks have been
previously distended with air, the Buccinator muscles expel it from between the
lips, as in blowing a trumpet; hence the name (buccina, a trumpet).
4.13 Category
4.13.1
Facial Expression (FE)
4.14 View
4.14.1
Anterior
4.14.1.1Illus. (DSL)
5 BULBOCAVERNOSUS
(BULBOSPONGIOSUS) B17E17
Back Table of Contents References
5.1 Word Derivation
5.1.1 Bulbus=Bulb
5.1.2 Caverna=Hollow
5.2 Attachments
5.2.1 Origin
5.2.1.1
Central tendon of perineum
5.2.2 Insertion
5.2.2.1
Inferior fascia of urogenital diaphragm
5.2.2.2
Corpus spongiosum of penis
5.2.2.3
Deep fascia on dorsum of penis in male
5.2.2.4
Pubic arch (Female)
5.2.2.5
Root and dorsum of clitoris (Female)
5.3 Action Illus. (DSL)
5.3.1 Helps expel last
drops of urine during micturition
5.3.2 Propel semen along
urethra
5.3.3 Assist in erection
of the penis in male
5.3.4 Decreases vaginal
orifice and assists in erection of clitoris in female
5.4 Nerve Supply
5.4.1 Perineal branch of
pudendal nerve
5.5 Synergists
5.5.1
5.6 Muscle Tests
5.6.1 BULBOCAVERNOSUS
5.7 Trigger Points
5.7.1 BULBOCAVERNOSUS
5.8 Organ Reflexes
5.8.1 None
5.8.2 Illustrations
5.9 Meridian
5.9.1 None
5.10 Discussion (Gray)
5.10.1
The Bulbocavernosus (Ejaculator
urinæ; Accelerator urinæ) (Fig. 406) is placed in the middle line of the perineum, in front of
the anus. It consists of two symmetrical parts, united along the median line by
a tendinous raphé. It arises from the central tendinous point of the
perineum and from the median raphé in front. Its fibers diverge like the barbs
of a quill-pen; the most posterior form a thin layer, which is lost on the
inferior fascia of the urogenital diaphragm; the middle fibers encircle the
bulb and adjacent parts, of the corpus cavernosum urethræ, and join with the
fibers of the opposite side, on the upper part of the corpus cavernosum
urethræ, in a strong aponeurosis; the anterior fibers, spread out over the side
of the corpus cavernosum penis, to be inserted partly into that body, anterior
to the Ischiocavernosus, occasionally extending to the pubis, and partly ending
in a tendinous expansion which covers the dorsal vessels of the penis. Dividing
the muscle longitudinally, and reflecting it from the surface of the corpus
cavernosum urethræ best see the latter fibers.
5.10.2
Actions—This muscle
serves to empty the canal of the urethra, after the bladder has expelled its
contents; during the greater part of the act of micturition its fibers are
relaxed, and it only comes into action at the end of the process. The middle
fibers are supposed by Krause to assist in the erection of the corpus
cavernosum urethræ, by compressing the erectile tissue of the bulb. The
anterior fibers, according to Tyrrel, also contribute to the erection of the
penis by compressing the deep dorsal vein of the penis, as they are inserted
into, and continuous with, the fascia of the penis.
5.11 Category
5.11.1
Perineum (PRN)
5.12 View
5.12.1
Ventral
5.12.1.1Illus. (DSL)
6 CILIARY MUSCLE B18E18
Back Table of Contents References
6.1 Attachments
6.1.1 Origin
6.1.1.1
Scleral spur (posterior margin)
6.1.2 Insertion
6.1.2.1
Stroma of the choroid
6.1.2.2
Ciliary processes
6.1.2.3
Orbiculus ciliaris
6.2 Action Illus. (DSL)
6.2.1 Modify
the shape of the lens to adjust for near (lens thickening) or distant Vision
(lens thinning)
6.3 Nerve Supply
6.3.1 Near
vision
6.3.1.1
Parasympathetic fibers through the Oculomotor
nerve (III), from Edinger-Westphal nucleus
6.3.2 Distant vision
6.3.2.1
Sympathetic fibers from the superior cervical ganglion
passing into the eye as the long ciliary nerves
6.4 Arterial supply
6.4.1 Long
posterior and anterior ciliary rami from the ophthalmic and lacrimal branches
of the internal carotid artery
6.5 Synergists
6.5.1 None
6.6 Muscle Tests
6.6.1 CILIARY
6.7 Trigger Points
6.7.1 CILIARY
6.8 Organ Reflexes
6.8.1 None
6.8.2 Illustrations
6.9 Meridian
6.9.1 None
6.10 Antagonists
6.10.1
Parasympathetic and Sympathetic
fibers produce antagonistic effects
6.10.2
Parasympathetic fibers
6.10.2.1
Contract the ciliary muscle thereby relaxing the zonal
fibers which suspend the lens at its periphery
6.10.2.2
The relaxed lens thickens
6.10.3
Sympathetic fibers
6.10.3.1
Act upon arteries in ciliary body
6.10.3.2
Vasomotor activity increases tension
in lens zonal fibers and produces a thinning of the lens
6.11 Discussion (Gray)
6.11.1
The Ciliaris muscle (m. ciliaris;
Bowman’s muscle) consists of unstriped fibers: it forms a grayish,
semitransparent, circular band, about 3 mm. broad, on the outer surface of the
forepart of the choroid. It is thickest in front, and consists of two sets of
fibers, meridional and circular. The meridional fibers, much the more numerous, arise from
the posterior margin of the scleral spur (page 1007); they run backward, and
are attached to the ciliary processes (Fig. 875) and orbiculus ciliaris (Fig. 875). One
bundle, according to Waldeyer, is inserted into the sclera. The circular fibers
are internal to the meridional ones, and in a meridional section appear as a
triangular zone behind the filtration angle and close to the circumference of
the iris. They are well developed in hypermetropic, but are rudimentary or
absent in myopic eyes. The Ciliaris muscle is the chief agent in accommodation,
i.e., in adjusting the eye to the vision of near objects. When it
contracts it, draws forward the ciliary processes, relaxes the suspensory
ligament of the lens, and thus allows the lens to become more convex.
6.11.2
Definitions
6.11.2.1
The Ciliary Body (corpus
ciliare)
—The ciliary body comprises the orbiculus
ciliaris,
and the Ciliaris muscle
6.11.2.2
The orbiculus ciliaris is a zone of
about 4 mm. in width, directly continuous with the anterior part of the
choroid; it presents numerous ridges arranged in a radial manner), the ciliary processes.
6.11.2.3
The ciliary processes (processus
ciliares) are formed by the inward folding of the various layers of the
choroid, i.e., the choroid proper and the lamina basalis, and are
received between corresponding foldings of the suspensory ligament of the lens.
6.11.2.4
Stroma of the choroid Interspersed
between the vessels are dark star-shaped pigment cells, the processes of which,
communicating with those of neighbouring cells, form a delicate net-work or
stroma, which toward the inner surface of the choroid loses its pigmentary
character. The inner layer (lamina
choriocapillaris) consists of an exceedingly fine capillary plexus, formed
by the short ciliary vessels; the network is closer and finer in the posterior
than in the anterior part of the choroid. About 1.25 cm. behind the cornea its
meshes become larger, and are continuous with those of the ciliary processes.
This lamina is connected by a stratum
intermedium
consisting of fine elastic fibers. On the inner surface of the lamina
choriocapillaris is a very thin, structureless, or faintly fibrous membrane,
called the lamina basalis; it is closely
connected with the stroma of the choroid, and separates it from the pigmentary
layer of the retina.
6.11.2.5
The Sclera —The sclera has
received its name from its extreme density and hardness; it is a firm,
unyielding membrane, serving to maintain the form of the bulb. It is much
thicker behind than in front; the thickness of its posterior part is 1 mm.
6.11.2.6
The Cornea —The cornea is
the projecting transparent part of the external tunic, and forms the anterior
sixth of the surface of the bulb.
6.11.2.7
The Iris —The iris has
received its name from its various colors in different individuals. It is a
thin, circular, contractile disk, suspended in the aqueous humour between the
cornea and lens, and perforated a little to the nasal side of its center by a
circular aperture, the pupil.
6.11.3
Additional Illustrations
6.11.3.1
(Fig. 869)
6.11.3.2
(Fig. 870)
6.11.3.3
(Fig. 872)
6.11.3.4
(Fig. 873)
6.11.3.5
(Fig. 874)
6.11.3.6
(Fig. 875)
6.11.3.7
(Fig.876)
6.12 Category
6.12.1
Eye Ball (EB)
6.13 View
6.13.1
(Note: Lower two s are enlarged horizontal
sections.)
6.13.1.1Illus. (DSL)
7 COCCYGEUS
(ISCHIOCOCCYGEUS) B19E19
Back Table of Contents References
7.1 Word Derivation
7.1.1 Coccygeus=Coccyx
7.2 Attachments Illus. 1 (DSL) Illus. 2 (DSL)
7.2.1 Origin
7.2.1.1
Ischial Spine
7.2.2 Insertion
7.2.2.1
Lower Sacrum
7.2.2.2
Upper Coccyx
7.3 Action Illus. (DSL)
7.3.1 Supports and
slightly raises pelvic floor
7.3.2 Resists
intraabdominal pressure
7.3.3 Pulls coccyx
forward following defecation or parturition
7.4 Nerve Supply
7.4.1 Nerve
7.4.1.1
Sacral
7.4.2 Roots
7.4.2.1
S3
7.4.2.2
S4
7.5 Synergists
7.5.1
7.6 Muscle Tests
7.6.1 COCCYGEUS
7.7 Trigger Points
7.7.1 COCCYGEUS
7.8 Organ Reflexes
7.8.1 None
7.8.2 Illustrations
7.9 Meridian
7.9.1 None
7.10 Discussion (Gray)
7.10.1
The Coccygeus (Fig. 404) is situated behind the preceding. It is a
triangular plane of muscular and tendinous fibers, arising by its apex
from the spine of the ischium and sacrospinous ligament, and inserted by
its base into the margin of the coccyx and into the side of the lowest piece of
the sacrum. It assists the Levator Ani and Piriformis in closing in the back
part of the outlet of the pelvis.
7.10.2
Nerve Supply —a branch from
the fourth and fifth sacral nerves supplies The Coccygeus.
7.10.3
Actions—The Coccygei pull
forward and support the coccyx, after it has been pressed backward during
defecation or parturition.
7.11 Category
7.11.1
Pelvic Floor (PF)
7.12 View
7.12.1
Ventral
7.12.1.1Illus. (DSL)
8 CORACOBRACHIALIS B20E20
Back Table of Contents References
8.1 Word Derivation
8.1.1 Coraco=Coracoid
process
8.2 Attachments Illus. (DSL)
8.2.1 Origin
8.2.1.1
Tip of coracoid process of scapula
8.2.2 Insertion
8.2.2.1
Middle of medial border of humerus,
opposite deltoid tuberosity
8.3 Joints
8.3.1 Glenohumeral
8.4 Action Illus. (DSL)
8.4.1 Horizontal
flexion
8.4.2 Adduction
8.5 Nerve Supply
8.5.1 Nerve
8.5.1.1
Musculocutaneous
8.5.2 Roots
8.5.2.1
C5
8.5.2.2
C6
8.5.2.3
C7
8.6 Synergists
8.6.1 Pectoralis
major
8.6.2 Biceps
brachii
8.6.3 Anterior
deltoid
8.7 Muscle Tests
8.7.1 CORACOBRACHIALIS
8.8 Trigger Points
8.8.1 CORACOBRACHIALIS
8.9 Organ Reflexes
8.9.1 Lung
8.9.2 Illustrations
8.10 Meridian
8.10.1
Lung
8.11 Discussion (Gray)
8.11.1
The Coracobrachialis (Fig. 411) the smallest of the three muscles in this region
is situated at the upper and medial part of the arm. It arises from the
apex of the coracoid process, in common with the short head of the Biceps
brachii, and from the intermuscular septum between the two muscles; it is inserted
by means of a flat tendon into an impression at the middle of the medial
surface and border of the body of the humerus between the origins of the
Triceps brachii and Brachialis. It is perforated by the musculocutaneous nerve
8.11.2
Variations —A bony head may
reach the medial epicondyle; a short head more rarely found may insert into the
lesser tubercle.
8.11.3
Actions —The
Coracobrachialis draws the humerus forward and medialward, and at the same time
assists in retaining the head of the bone in contact with the glenoid cavity.
8.12 Category
8.12.1
Arm Scapular (AS)
8.13 View
8.13.1
Anterior
8.13.1.1Illus. (DSL)
9 CORRUGATOR
SUPERCILII B21E21
Back Table of Contents References
9.1 Word Derivation
9.1.1 Corrugo=Wrinkle
9.1.2 Supercilium=Eyebrow
9.2 Attachments
9.3
Origin
9.3.1.1
Medial end of the superciliary arch of
the frontal bone
9.4
Insertion
9.4.1.1
Deep surface of the skin above the
midpart of the orbital arch
9.5 Action Illus. (DSL)
9.5.1 :
Draws eyebrows medially and down (Frowning muscle)
9.6 Nerve Supply
9.6.1 Temporal
branches of the facial nerve (VII)
9.7 Artery supply
9.7.1 Supratrochlear
(Branch of ophthalmic)
9.7.2 Supraorbital
(Branch of ophthalmic)
9.8 Synergists
9.8.1 Orbicularis
oculi
9.8.2 Procerus
9.9 Antagonist
9.9.1 Frontalis
9.10 Muscle Tests
9.10.1
CORRUGATOR SUPERCILII
9.11 Trigger Points
9.11.1
CORRUGATOR SUPERCILII
9.12 Organ Reflexes
9.12.1
None
9.12.2
Illustrations
9.13 Meridian
9.13.1
None
9.14 Discussion (Gray)
9.14.1
The Corrugator (Corrugator
supercilii) (Fig. 379) is a small, narrow,
pyramidal muscle, placed at the medial end of the eyebrow, beneath the
Frontalis and Orbicularis oculi. It arises from the medial end of the
superciliary arch; and its fibers pass upward and lateralward, between the
palpebral and orbital portions of the Orbicularis oculi, and is inserted
into the deep surface of the skin, above the middle of the orbital arch.
9.14.2
Note 79 The
corrugator is not recognized as a separate muscle in the Basle Nomenclature.
9.14.3
Actions- The Corrugator
draws the eyebrow downward and medialward, producing the vertical wrinkles of
the forehead. It is the “frowning” muscle, and may be regarded as the principal
muscle in the expression of suffering.
9.15 Category
9.15.1
Facial Expression (FE)
9.16 View
9.16.1
Anterior
9.16.1.1Illus. (DSL)
10 CRICOARYTENOID
LATERAL & POSTERIOR B22E22
Back Table of Contents References
10.1 Attachments Illus. (DSL)
10.1.1
Origin
10.1.1.1Cricoarytenoid Lateral
10.1.1.1.1
Upper
border of arch of cricoid cartilage
10.1.1.2Cricoarytenoid Posterior
10.1.1.2.1
Posterior
surface of lamina of cricoid cartilage
10.1.2
Insertion
10.1.2.1Cricoarytenoid Lateral
10.1.2.1.1
Muscular
process of arytenoids cartilage
10.1.2.2Cricoarytenoid Posterior
10.1.2.2.1
Muscular
process of arytenoid cartilage
10.2 Action Illus. (DSL)
10.2.1
Cricoarytenoid Lateral
10.2.1.1
Adducts and medially rotates arytenoid cartilage assisting
in closing glottis
10.2.2
Cricoarytenoid Posterior
10.2.2.1
Abducts arytenoid cartilage widening glottis
10.3 Nerve Supply
10.3.1
Vagus (X)
10.3.2
Accessory (XI)
10.4 Synergists
10.4.1
10.5 Muscle Tests
10.5.1
CRICOARYTENOID
10.6 Trigger Points
10.6.1
CRICOARYTENOID
10.7 Organ Reflexes
10.7.1
None
10.7.2
Illustrations
10.8 Meridian
10.8.1
None
10.9 Discussion (Gray)
10.9.1
The Cricoarytænoideus
posterior
(posterior cricoarytenoid) (Fig. 958) arises from the broad depression on the
corresponding half of the posterior surface of the lamina of the cricoid cartilage;
its fibers run upward and lateralward, and converge to be inserted into
the back of the muscular process of the arytenoid cartilage. The uppermost
fibers are nearly horizontal, the middle oblique, and the lowest almost
vertical.
10.9.2
Actions-The Cricoarytœnoidei posteriores separate the
vocal folds, and, consequently, open the glottis, by rotating the arytenoid
cartilages outward around a vertical axis passing through the cricoarytenoid
joints; so that their vocal processes and the vocal folds attached to them
become widely separated.
10.9.3
The Cricoarytænoideus
lateralis
(lateral cricoarytenoid) (Fig. 959) is smaller than the preceding, and of an oblong
form. It arises from the upper border of the arch of the cricoid
cartilage, and, passing obliquely upward and backward, is inserted into the
front of the muscular process of the arytenoid cartilage.
10.9.4
Actions-The Cricoarytœnoidei laterales close the
glottis by rotating the arytenoid cartilages inward, to approximate their vocal
processes.
10.10
Category
10.10.1
Larynx Intrinsic (LXI)
10.11
View
10.11.1
LATERAL AND POSTERIOR VIEW
10.11.1.1 Illus. (DSL)
11 CRICOPHARYNGEUS B23E23
Back Table of Contents References
11.1 Attachments
11.1.1
Origin
11.1.1.1Arch of cricoid cartilage
11.1.2
Insertion
11.1.2.1Arch of cricoid cartilage
11.2 Action Illus. (DSL)
11.2.1
Acts as sphincter to prevent air entering esophagus
11.2.2
Relaxes during swallowing
11.3 Nerve Supply
11.3.1
Nerve Plexus
11.3.1.1
Pharyngeal plexus
11.3.2
Roots
11.3.2.1
CN (IX)
11.3.2.2
CN (X)
11.3.2.3
CN (XI)
11.4 Synergists
11.4.1
11.5 Muscle Tests
11.5.1
CRICOPHARYNGEUS
11.6 Trigger Points
11.6.1
CRICOPHARYNGEUS
11.7 Organ Reflexes
11.7.1
None
11.7.2
Illustrations
11.8 Meridian
11.8.1
None
11.9 Discussion (Gray)
11.9.1
None
11.10
Category
11.10.1
Pharynx longitudinal layer (PXL)
11.11
View
11.11.1
Posterior
11.11.1.1 Illus. (DSL)
12 CRICOTHYROID B24E24
Back Table of Contents References
12.1 Word Derivation
12.1.1
Crico=Cricoid cartilage of larynx
12.1.2
Thyro=Thyroid gland
12.2 Attachments
12.2.1
Origin
12.2.1.1Anterolateral,
external aspect of the cricoid cartilage
12.2.2
Insertion
12.2.2.1Inferior
part
12.2.2.1.1
Anterior
border of the inferior cornu of thyroid
12.2.2.2Superior
Part
12.2.2.2.1
Posterior
part of the lower border of the thyroid lamina
12.3 Action Illus. (DSL)
12.3.1
Elevation of cricoid arch and
tilting, back its lamina
12.3.2
Closes anterior interval between the
cricoid and thyroid cartilages, thereby, tightening the vocal cords
12.4 Nerve Supply
12.4.1
External branch of the superior
laryngeal nerve from the vagus nerve (X)
12.5 Arterial
supply
12.5.1
Cricothyroid branch and rami of the
superior thyroid artery
12.5.2
Rami from the inferior thyroid artery
12.6 Synergists
12.6.1
Posterior Arytenoids
12.7 Antagonists
12.7.1
Vocalis
12.7.2
Thyroarytenoid
12.8 Muscle Tests
12.8.1
CRICOTHYROID
12.9 Trigger Points
12.9.1
CRICOTHYROID
12.10
Organ Reflexes
12.10.1
None
12.10.2
Illustrations
12.11
Meridian
12.11.1
None
12.12
Discussion (Gray)
12.12.1
The Cricothyreoideus (Cricothyroid)
(Fig. 957), triangular in form, arises from the front
and lateral part of the cricoid cartilage; its fibers diverge, and are arranged
in two groups. The lower fibers constitute a pars
obliqua,
slant backward, and lateralward to the anterior border of the inferior cornu;
the anterior fibers, forming pars recta, run upward,
backward, and lateralward to the posterior part of the lower border of the
lamina of the thyroid cartilage. The medial borders of the two muscles are
separated by a triangular interval, occupied by the middle cricothyroid
ligament.
12.12.2
The medial borders of the two muscles are separated by a
triangular interval, occupied by the middle cricothyroid ligament.
12.12.3
The Cricothyreoideus produce tension and elongation
of the vocal folds by drawing up the arch of the cricoid cartilage and tilting
back the upper border of its lamina; the distance between the vocal processes
and the angle of the thyroid is thus increased, and the folds are consequently
elongated.
12.12.4
Actions-
12.12.4.1 The
Cricoarytœnoidei posteriores separate the vocal folds, and, consequently, open
the glottis, by rotating the arytenoid cartilages outward around a vertical
axis passing through the cricoarytenoid joints; so that their vocal processes
and the vocal folds attached to them become widely separated.
12.12.4.2 The Cricoarytœnoidei
laterales close the glottis by rotating the arytenoid cartilages inward, to
approximate their vocal processes.
12.13
Category
12.13.1
Larynx Intrinsic (LXI)
12.14
View
12.14.1
Posterior
12.14.1.1 Illus. (DSL)
13 DELTOID ANTERIOR
B25E25
Back Table of Contents References
13.1 Word Derivation
13.1.1
Delta=Triangular
13.1.2
Supercilium=Eyebrow
13.2 Attachments Illus.
(DSL)
13.2.1
Origin
13.2.1.1 Anterosuperior
border of the lateral 1/3 of the clavicle
13.2.2
Insertion
13.2.2.1 Deltoid
tuberosity of the humerus on the anterolateral surface just above is midshaft
13.3 Joints
13.3.1
Glenohumeral
13.4 Action Illus.
(DSL)
13.4.1
Abduction
13.4.2
Horizontal flexion
13.4.3
Medial rotation
13.5 Nerve Supply
13.5.1
Nerve
13.5.1.1
Axillary
13.5.2
Roots
13.5.2.1
C5
13.5.2.2
C6
13.6 Synergists
13.6.1
Middle Deltoid
13.6.2
Posterior Deltoid
13.6.3
Supraspinatus
13.6.4
Pectoralis Major Clavicular
13.7 Muscle Tests
13.7.1
DELTOID ANTERIOR
13.8 Trigger Points
13.8.1
DELTOID ANTERIOR
13.9 Organ Reflexes
13.9.1
Lung
13.9.2
Illustrations
13.10
Meridian
13.10.1 Lung
13.11
Discussion (Gray)
13.11.1 The Deltoideus (Deltoid muscle) (Fig. 410) is a large, thick, triangular muscle, which covers the
shoulder-joint in front, behind, and laterally. It arises from the
anterior border and upper surface of the lateral third of the clavicle, from
the lateral margin and upper surface of the acromion, and from the lower lip of
the posterior border of the spine of the scapula, as far back as the triangular
surface at its medial end. From this extensive origin the fibers converge
toward their insertion, the middle passing vertically, the anterior obliquely backward
and lateralward, the posterior obliquely forward and lateralward; they unite in
a thick tendon, which is inserted into the deltoid prominence on the middle of
the lateral side of the body of the humerus. At its insertion, the
muscle gives off an expansion to the deep fascia of the arm. This muscle is
remarkably coarse in texture, and the arrangement of its fibers is somewhat
peculiar; the central portion of the muscle—that is to say, the part arising
from the acromion—consists of oblique fibers; these arise in a bipenniform
manner from the sides of the tendinous intersections, generally four in number,
which are attached above to the acromion and pass downward parallel to one
another in the substance of the muscle. The oblique fibers thus formed are inserted
into similar tendinous intersections, generally three in number, which pass
upward from the insertion of the muscle and alternate with the descending
septa. The portions of the muscle arising from the clavicle and spine of the
scapula are not arranged in this manner, but are inserted into the margins of
the inferior tendon.
13.11.2 Variations —Large variations
uncommon. More or less splitting common. Continuation into the Trapezius;
fusion with the Pectoralis major; additional slips from the vertebral border of
the scapula, infraspinous fascia and axillary border of scapula not uncommon.
Insertion varies in extent or rarely is prolonged to origin of Brachioradialis.
13.11.3 Nerves —The Deltoideus
is supplied by the fifth and sixth cervical through the axillary nerve.
13.11.4 Actions —The Deltoideus
raises the arm from the side, to bring it at right angles with the trunk. Its
anterior fibers, assisted by the Pectoralis major, draw the arm forward; and
its posterior fibers, aided by the Teres major and Latissimus dorsi, draw it
backward.
13.11.5 Illustration-None
13.12
Category
13.12.1 Arm
Scapular (AS)
13.13
View
13.13.1 Anterior
13.13.1.1 Illus. (DSL)
14 DELTOID MIDDLE
Back Table of Contents References
14.1 Origin
14.1.1
Superior surface of the Acromion
process
14.2 Insertion
14.2.1
Deltoid tuberosity of humerus
14.3 Joints
14.3.1
Glenohumeral
14.4 Action
14.4.1
Abduction
14.5 Nerve Supply
14.5.1
Nerve
14.5.1.1Axillary
14.5.2
Roots
14.5.2.1C5
14.5.2.2C6
14.6 Synergists
14.6.1
Anterior Deltoid
14.6.2
Posterior Deltoid
14.6.3
Supraspinatus
14.7 Category
14.7.1
Arm Scapular (AS)
15 DELTOID POSTERIOR
Back Table of Contents References
15.1 Origin
15.1.1
Inferior margin of spine of scapula
15.2 Insertion
15.2.1
Deltoid tuberosity of humerus
15.3 Joints
15.3.1
Glenohumeral
15.4 Action
15.4.1
Abduction
15.4.2
Horizontal Extension
15.4.3
Lateral Rotation
15.5 Nerve Supply
15.5.1
Nerve
15.5.1.1Axillary
15.5.2
Roots
15.5.2.1C5
15.5.2.2C6
15.6 Synergists
15.6.1
Anterior Deltoid
15.6.2
Middle Deltoid
15.6.3
Supraspinatus
15.7 Category
15.7.1
Arm Scapular (AS)
16 DEPRESSOR ANGULI
ORIS
Back Table of Contents References
16.1 Origin
16.1.1
The
oblique line of the mandible, below and lateral to the depressor labii
inferioris
16.2 Insertion
16.2.1
The
angle of the mouth, mingling with the levator anguli oris, zygomatIcus major,
and muscular bands of the orbicularis Oris
16.3 Action
16.3.1
Depresses
the modiolus and angle of mouth
16.4 Nerve Supply
16.4.1
Mandibular
marginal branch of the facial nerve (VII)
16.5 Arterial supply
16.5.1
Inferior
labial branch from the facial artery
16.5.2
Mental
branch from the inferior alveolar artery
16.6 Synergists
16.6.1
Platysma
(Pars Modiolus)
16.6.2
Depressor
Labii Inferioris
16.7 Antagonists
16.7.1
For
direct modiolar deviation
16.7.1.1Levator Anguli Oris
16.7.1.2Zygomaticus Major
16.7.2
For
angle of mouth deviation
16.7.2.1Lateral Slip of the Levator Labii
Superioris
16.7.2.2Alaeque Nasi
16.7.2.3Levator Labii Superioris
16.7.2.4Zygomaticus Minor
16.8 Category
16.8.1
Facial Expression (FE)
16.9 Note
16.9.1
(Denotes
Modiolus)
17 DEPRESSOR LABII
INFERIORIS
17.1 Origin
17.1.1
The
oblique line of mandible, between symphysis menti and the mental foramen
17.2 Insertion
17.2.1
The
skin of the lower lip, blending and intersecting with its other and with
orbicularis oris
17.2.2
Note
17.2.2.1It
is
continuous below and laterally with the labial part of the platysma).
17.3 Action
17.3.1
Depresses
the lower lip laterally and assists in eversion
17.4 Nerve Supply
17.4.1
Mandibular
marginal branch of the facial nerve (VII)
17.5 Arterial supply
17.5.1
Inferior
labial branch of the facial artery
17.5.2
Mental
branch of the inferior alveolar artery
17.6 Synergists
17.6.1
Platysma
(Pars Labialis)
17.6.2
Depressor
Anguli Oris
17.7 Antagonist
17.7.1
Orbicularis
Oris
17.8 Category
17.8.1
Facial Expression (FE)
18 DEPRESSOR SEPTI
18.1 Origin
18.1.1
From
the incisive fossa of the maxilla
18.2 Insertion
18.2.1
The
mobile part of the nasal septum, deep to the superior labial mucous membrane
18.3 Action
18.3.1
Draws
ala of nose downwards and thereby constricts the aperture of naris.
18.4 Nerve Supply
18.4.1
Superior
buccal branches of the facial nerve (VII)
18.5 Arterial supply
18.5.1
Septal
and alar branches from the superior labial artery
18.6 Synergists
18.6.1
Nasalis
18.7 Antagonist
18.7.1
Dilator
Naris
18.8 Category
18.8.1
Facial Expression (FE)
19 DIAPHRAGM
19.1 Word
Derivation/Pronunciation ect
19.1.1
http://www.m-w.com/dictionary/DIAPHRAGM
19.2 Origin
19.2.1
An approximately circular line
passing entirely around the inner surface of the body wall
19.2.2
STERNAL PORTION
19.2.2.1Two
slips from the back of the xiphoid process
19.2.3
COSTAL PORTION
19.2.3.1The
inner surfaces of the cartilages and adjacent portions of the lower 6 ribs on
either side, interdigitating with the transverses abdominis
19.2.4
LUMBAR PORTION
19.2.4.1Medial
(Medial Lumbocostal Arch) and lateral arcuate (Lateral Lumbocostal Arch) ligaments
and right and left crura from the anterolateral surfaces of the bodies and
discs of the upper three lumbar vertebrae
19.3 Insertion
19.3.1
The central tendon, which is an
oblong sheet forming the summit of the dome
19.4 Action
19.4.1
Principal muscle of respiration
19.4.2
Draws the central tendon downward,
during quiet inspiration, pressing against the abdominal visera
19.5 Nerve Supply
19.5.1
Nerve
19.5.1.1Phrenic
(Cervical Plexus)
19.5.2
Roots
19.5.2.1C3
19.5.2.2C4
19.5.2.3C5
19.6 Synergists
19.6.1
External Intercostals
19.6.2
Internal Intercostals
19.6.3
Serratus Posterior Superior
19.6.4
Scalenus Anterior
19.6.5
Scalenus Medius
19.6.6
Scalenus Posterior
19.6.7
Levatores Costarum
19.7 Discussion (Gray)
19.7.1
The Diaphragm (Fig. 391) is a dome-shaped musculofibrous septum which separates
the thoracic from the abdominal cavity, its convex upper surface forming the
floor of the former, and its concave under surface the roof of the latter. Its
peripheral part consists of muscular fibers which take origin from the
circumference of the thoracic outlet and converge to be inserted into a central
tendon. 15
19.7.2
The muscular fibers
may be grouped according to their origins into three parts—sternal, costal, and
lumbar. The sternal part arises by two fleshy slips from the back of the
xiphoid process; the costal part from the inner surfaces of the cartilages and
adjacent portions of the lower six ribs on either side, interdigitating with
the Transversus abdominis; and the lumbar part from aponeurotic arches, named
the lumbocostal arches, and from the lumbar vertebræ by two pillars or crura.
There are two lumbocostal arches, a medial and a lateral, on either side. 16
19.7.3
The Medial
Lumbocostal Arch (arcus lumbocostalis medialis [Halleri]; internal arcuate
ligament) is a tendinous arch in the fascia covering the upper part of the
Psoas major; medially, it is continuous with the lateral tendinous margin of
the corresponding crus, and is attached to the side of the body of the first or
second lumbar vertebra; laterally, it is fixed to the front of the transverse
process of the first and, sometimes also, to that of the second lumbar
vertebra. 17
19.7.4
The Lateral
Lumbocostal Arch (arcus lumbocostalis lateralis [Halleri]; external arcuate
ligament) arches across the upper part of the Quadratus lumborum, and is
attached, medially, to the front of the transverse process of the first lumbar
vertebra, and, laterally, to the tip and lower margin of the twelfth rib. 18
19.7.5
The Crura.—At their origins the crura are tendinous in
structure, and blend with the anterior longitudinal ligament of the vertebral
column. The right crus, larger and longer than the left, arises from the
anterior surfaces of the bodies and intervertebral fibrocartilages of the upper
three lumbar vertebræ, while the left crus arises from the corresponding parts
of the upper two only. The medial tendinous margins of the crura pass forward
and medialward, and meet in the middle line to form an arch across the front of
the aorta; this arch is often poorly defined.
19
19.7.6
From this series of
origins the fibers of the diaphragm converge to be inserted into the central
tendon. The fibers arising from the xiphoid process are very short, and
occasionally aponeurotic; those from the medial and lateral lumbocostal arches,
and more especially those from the ribs and their cartilages, are longer, and
describe marked curves as they ascend and converge to their insertion. The
fibers of the crura diverge as they ascend, the most lateral being directed
upward and lateralward to the central tendon. The medial fibers of the right
crus ascend on the left side of the esophageal hiatus, and occasionally a
fasciculus of the left crus crosses the aorta and runs obliquely through the
fibers of the right crus toward the vena caval foramen (Low 82).
20
19.7.7
The Central Tendon.—The central tendon of the diaphragm is a
thin but strong aponeurosis situated near the center of the vault formed by the
muscle, but somewhat closer to the front than to the back of the thorax, so
that the posterior muscular fibers are the longer. It is situated immediately
below the pericardium, with which it is partially blended. It is shaped
somewhat like a trefoil leaf, consisting
of three divisions or leaflets separated from one another by slight
indentations. The right leaflet is the largest, the middle, directed toward the
xiphoid process, the next in size, and the left the smallest. In structure the
tendon is composed of several planes of fibers, which intersect one another at
various angles and unite into straight or curved bundles—an arrangement which
gives it additional strength. 21
19.7.8
Openings in the Diaphragm.—The diaphragm is pierced by a
series of apertures to permit of the passage of structures between the thorax
and abdomen. Three large openings—the aortic, the esophageal, and the vena
caval—and a series of smaller ones are described. 22
19.7.9
The aortic hiatus is
the lowest and most posterior of the large apertures; it lies at the level of
the twelfth thoracic vertebra. Strictly speaking, it is not an aperture in the
diaphragm but an osseoaponeurotic opening between it and the vertebral column,
and therefore behind the diaphragm; occasionally some tendinous fibers
prolonged across the bodies of the vertebræ from the medial parts of the lower
ends of the crura pass behind the aorta, and thus convert the hiatus into a
fibrous ring. The hiatus is situated slightly to the left of the middle line,
and is bounded in front by the crura, and behind by the body of the first
lumbar vertebra. Through it pass the aorta, the azygos vein, and the thoracic
duct; occasionally the azygos vein is transmitted through the right crus. 23
19.7.10 The esophageal hiatus is situated in the
muscular part of the diaphragm at the level of the tenth thoracic vertebra, and
is elliptical in shape. It is placed above, in front, and a little to the left
of the aortic hiatus, and transmits the esophagus, the vagus nerves, and some
small esophageal arteries. 24
19.7.11 The vena caval foramen is the highest of the
three, and is situated about the level of the fibrocartilage between the eighth
and ninth thoracic vertebræ. It is quadrilateral in form, and is placed at the
junction of the right and middle leaflets of the central tendon, so that its
margins are tendinous. It transmits the inferior vena cava, the wall of which
is adherent to the margins of the opening, and some branches of the right
phrenic nerve. 25
19.7.12 Of the lesser apertures, two in the right
crus transmit the greater and lesser right splanchnic nerves; three in the left
crus give passage to the greater and lesser left splanchnic nerves and the
hemiazygos vein. The gangliated trunks of the sympathetic usually enter the
abdominal cavity behind the diaphragm, under the medial lumbocostal
arches. 26
19.7.13 On either side two small intervals exist at
which the muscular fibers of the diaphragm are deficient and are replaced by
areolar tissue. One between the sternal and costal parts transmits the superior
epigastric branch of the internal mammary artery and some lymphatics from the
abdominal wall and convex surface of the liver. The other, between the fibers
springing from the medial and lateral lumbocostal arches, is less constant;
when this interval exists, the upper and back part of the kidney is separated
from the pleura by areolar tissue only.
27
19.7.14 Variations.—The
sternal portion of the muscle is sometimes wanting and more rarely defects
occur in the lateral part of the central tendon or adjoining muscle
fibers. 28
19.7.15 Nerves.—The
diaphragm is supplied by the phrenic and lower intercostal nerves. 29
19.7.16 Actions.—The
diaphragm is the principal muscle of inspiration, and presents the form of a
dome concave toward the abdomen. The central part of the dome is tendinous, and
the pericardium is attached to its upper surface; the circumference is
muscular. During inspiration the lowest ribs are fixed, and from these and the
crura the muscular fibers contract and draw downward and forward the central
tendon with the attached pericardium. In this movement the curvature of the
diaphragm is scarcely altered, the dome moving downward nearly parallel to its
original position and pushing before it the abdominal viscera. The descent of
the abdominal viscera is permitted by the elasticity of the abdominal wall, but
the limit of this is soon reached. The central tendon applied to the abdominal
viscera then becomes a fixed point for the action of the diaphragm, the effect
of which is to elevate the lower ribs and through them to push forward the body
of the sternum and the upper ribs. The right cupola of the diaphragm, lying on
the liver, has a greater resistance to overcome than the left, which lies over
the stomach, but to compensate for this the right crus and the fibers of the
right side generally are stronger than those of the left. 30
19.7.17 In all expulsive acts the diaphragm is called
into action to give additional power to each expulsive effort. Thus, before
sneezing, coughing, laughing, crying, or vomiting, and previous to the
expulsion of urine or feces, or of the fetus from the uterus, a deep
inspiration takes place. The height of the diaphragm is constantly varying
during respiration; it also varies with the degree of distension of the stomach
and intestines and with the size of the liver. After a forced expiration the
right cupola is on a level in front with the fourth costal cartilage, at the
side with the fifth, sixth, and seventh ribs, and behind with the eighth rib;
the left cupola is a little lower than the right. Halls Dally 83 states that the absolute range of movement
between deep inspiration and deep expiration averages in the male and female 30
mm. on the right side and 28 mm. on the left; in quiet respiration the average
movement is 12.5 mm. on the right side and 12 mm. on the left. 31
19.7.18 Skiagraphy shows that the height of the
diaphragm in the thorax varies considerably with the position of the body. It
stands highest when the body is horizontal and the patient on his back, and in
this position it performs the largest respiratory excursions with normal
breathing. When the body is erect the dome of the diaphragm falls, and its
respiratory movements become smaller. The dome falls still lower when the
sitting posture is assumed, and in this position its respiratory excursions are
smallest. These facts may, perhaps, explain why it is that patients suffering
from severe dyspnœa are most comfortable and least short of breath when they
sit up. When the body is horizontal and the patient on his side, the two halves
of the diaphragm do not behave alike. The uppermost half sinks to a level lower
even than when the patient sits, and moves little with respiration; the lower
half rises higher in the thorax than it does when the patient is supine, and
its respiratory excursions are much increased. In unilateral disease of the
pleura or lungs analogous interference with the position or movement of the
diaphragm can generally be observed skiagraphically. 32
19.7.19 It appears that the position of the diaphragm
in the thorax depends upon three main factors, viz.: (1) the elastic retraction
of the lung tissue, tending to pull it upward; (2) the pressure exerted on its
under surface by the viscera; this naturally tends to be a negative pressure,
or downward suction, when the patient sits or stands, and positive, or an
upward pressure, when he lies; (3) the intra-abdominal tension due to the abdominal
muscles. These are in a state of contraction in the standing position and not
in the sitting; hence the diaphragm, when the patient stands, is pushed up
higher than when he sits. 33
19.7.20 The Intercostales interni and externi have
probably no action in moving the ribs. They contract simultaneously and form
strong elastic supports which prevent the intercostal spaces being pushed out
or drawn in during respiration. The anterior portions of the Intercostales
interni probably have an additional function in keeping the sternocostal and
interchondral joint surfaces in apposition, the posterior parts of the
Intercostales externi performing a similar function for the costovertebral
articulations. The Levatores costarum being inserted near the fulcra of the ribs
can have little action on the ribs; they act as rotators and lateral flexors of
the vertebral column. The Transversus thoracis draws down the costal
cartilages, and is therefore a muscle of expiration. 34
19.7.21 The Serrati are respiratory muscles. The Serratus
posterior superior elevates the ribs and is therefore an inspiratory muscle.
The Serratus posterior inferior draws the lower ribs downward and backward, and
thus elongates the thorax; it also fixes the lower ribs, thus assisting the
inspiratory action of the diaphragm and resisting the tendency it has to draw
the lower ribs upward and forward. It must therefore be regarded as a muscle of
inspiration. 35
19.7.22 Mechanism of
Respiration.—The respiratory movements must be examined during (a) quiet respiration,
and (b) deep respiration. 36
19.7.23 Quiet Respiration.—The first and second pairs
of ribs are fixed by the resistance of the cervical structures; the last pair,
and through it the eleventh, by the Quadratus lumborum. The other ribs are
elevated, so that the first two intercostal spaces are diminished while the
others are increased in width. It has already been shown (p. 304) that
elevation of the third, fourth, fifth, and sixth ribs leads to an increase in
the antero-posterior and transverse diameters of the thorax; the vertical
diameter is increased by the descent of the diaphragmatic dome so that the
lungs are expanded in all directions except backward and upward. Elevation of
the eighth, ninth, and tenth ribs is accompanied by a lateral and backward
movement, leading to an increase in the transverse diameter of the upper part
of the abdomen; the elasticity of the anterior abdominal wall allows a slight
increase in the antero-posterior diameter of this part, and in this way the
decrease in the vertical diameter of the abdomen is compensated and space
provided for its displaced viscera. Expiration is effected by the elastic
recoil of its walls and by the action of the abdominal muscles, which push back
the viscera displaced downward by the diaphragm. 37
19.7.24 Deep Respiration.—All the movements of quiet
respiration are here carried out, but to a greater extent. In deep inspiration
the shoulders and the vertebral borders of the scapulæ are fixed and the limb
muscles, Trapezius, Serratus anterior, Pectorales, and Latissimus dorsi, are
called into play. The Scaleni are in strong action, and the
Sternocleidomastoidei also assist when the head is fixed by drawing up the
sternum and by fixing the clavicles. The first rib is therefore no longer
stationary, but, with the sternum, is raised; with it all the other ribs except
the last are raised to a higher level. In conjunction with the increased
descent of the diaphragm this provides for a considerable augmentation of all
the thoracic diameters. The anterior abdominal muscles come into action so that
the umbilicus is drawn upward and backward, but this allows the diaphragm to
exert a more powerful influence on the lower ribs; the transverse diameter of
the upper part of the abdomen is greatly increased and the subcostal angle
opened out. The deeper muscles of the back, e.g., the Serrati posteriores
superiores and the Sacrospinales and their continuations, are also brought into
action; the thoracic curve of the vertebral column is partially straightened,
and the whole column, above the lower lumbar vertebræ, drawn backward. This
increases the antero-posterior diameters of the thorax and upper part of the
abdomen and widens the intercostal spaces. Deep expiration is effected by the
recoil of the walls and by the contraction of the antero-lateral muscles of the
abdominal wall, and the Serrati posteriores inferiores and Transversus
thoracis. 38
19.7.25 Halls Dally (op. cit.) gives the following
figures as representing the average changes which occur during deepest possible
respiration. The manubrium sterni moves 30 mm. in an upward and 14 mm. in a
forward direction; the width of the subcostal angle, at a level of 30 mm. below
the articulation between the body of the sternum and the xiphoid process, is
increased by 26 mm.; the umbilicus is retracted and drawn upward for a distance
of 13 mm.
19.8 Category
19.8.1
Breathing (B)
19.9 Iluustration
19.9.1
Grays
19.9.1.1http://www.bartleby.com/107/illus391.html
20 DIGASTRIC ANT
& POST BELLY (SUPRAHYOID)
20.1 Origin
20.1.1
Anterior
belly
20.1.1.1Digastric fossa of mandible
20.1.2
Posterior
belly
20.1.2.1Mastoid notch of temporal bone
20.2 Insertion
20.2.1
Intermediate
tendon attached to the hyoid via a fibrous loop
20.3 Action
20.3.1
Mandibular
depression and hyoid elevation
20.3.2
Note
20.3.2.1Both bellies act together during
swallowing and chewing
20.4 Nerve Supply
20.4.1
Anterior
belly
20.4.1.1Mylohyoid rami from the inferior
alveolar branch of the trIgeminal nerve (V3)
20.4.2
Posterior
belly
20.4.2.1Digastric branch facial nerve (VII)
20.5 Arterial supply
20.5.1
Anterior
belly
20.5.1.1Mylohyoid branch of inferior alveolar
artery
20.5.1.2Submandibular branch of the facial
artery
20.5.2
Posterior
belly
20.5.2.1Posterior auricular artery and muscular
branches of the occipital artery
20.6 Synergists
20.6.1
Mandibular
Depression
20.6.1.1Mylohyoid
20.6.1.2Geniohyoid
20.6.1.3Lateral Pterygoid
20.6.1.4Platysma
20.6.2
Hyoid
Elevation
20.6.2.1Stylohyoid
20.6.2.2Mylohyoid
20.6.2.3Geniohyoid
20.7 Antagonists
20.7.1
Mandibular
Depression
20.7.1.1Masseter
20.7.1.2Temporalis
20.7.1.3Medial Pterygoid
20.7.2
Hyoid
Elevation
20.7.2.1Sternohyoid
20.7.2.2Thyrohyoid
20.7.2.3Omohyoid
20.8 Category
20.8.1
ORAL CAVITY FLOOR (OCF)
21 DILATOR PUPILLAE
21.1 Origin
21.1.1
The
mesodermal stroma in the periphery of the iris
21.2 Insertion
21.2.1
The
iris among the outer parts of the sphincter pupillae fibers
21.3 Action
21.3.1
Dilation
of the pupil to adjust for distant vision or diminished light
21.4 Nerve Supply
21.4.1
Sympathetic
fibers from the superior cervical ganglion passing as long ciliary nerves to
the globe
21.5 Arterial supply
21.5.1
Long
posterior and anterior ciliary rami from the ophthalmic and lacrimal branches
of the internal carotid artery
21.6 Synergists
21.6.1
None
21.7 Antagonist
21.7.1
Sphincter
pupillae
21.8 Category
21.8.1
Eye Ball (EB)
21.9 View
21.9.1
Note
21.9.1.1Lower 2 s are enlarged horizontal
sections
22 DORSAL INTEROSSEI
(FOOT)
Back Table of Contents References
22.1 Attachments
22.1.1
Origin
22.1.1.1 There
are four dorsal Interossei each by two heads from adjacent sides of the
metatarsals
22.1.2
Insertion
22.1.2.1Bases
of the proximal phalanges
22.1.2.2Extensor
expansion of the tendons of the extensor digitorum longus
22.1.2.3The
1st dorsal interosseous (arising from the 1st and 2nd metatarsals) inserts into
the medial side of the 2nd toe
22.1.2.4The
2nd-4th dorsal Interossei insert into the lateral sides of the 2nd 3rd and 4th
toes
22.2 Action
22.2.1
Abducts the 2nd, 3rd and 4th toes
away from the longitudinal axis of the 2nd toe
22.2.2
Assists in flexing the proximal
phalanx
22.2.3
Extends the middle and distal
phalanges
22.3 Nerve Supply
22.3.1
Nerve
22.3.1.1Lateral
Plantar
22.3.2
Roots
22.3.2.1S2
22.3.2.2S3
22.4 Synergists
22.4.1
Plantar Interossei
22.5 Muscle
Tests
22.5.1
22.6 Trigger Points
22.6.1
22.7 Discussion (Gray)
22.7.1
Interossei—The Interossei in the foot are similar to those in
the hand, with this exception, that they are grouped around the middle line of
the second digit, instead of that of the third. They are seven in number, and
consist of two groups, dorsal and plantar.
29
22.7.2
The Interossei
dorsales (Dorsal interossei) (Fig. 446), four in number, are situated between
the metatarsal bones. They are bipenniform muscles, each arising by two heads
from the adjacent sides of the metatarsal bones between which it is placed;
their tendons are inserted into the bases of the first phalanges, and into the
aponeurosis of the tendons of the Extensor digitorum longus. In the angular
interval left between the heads of each of the three lateral muscles, one of
the perforating arteries passes to the dorsum of the foot; through the space between
the heads of the first muscle the deep plantar branch of the dorsalis pedis
artery enters the sole of the foot. The first is inserted into the medial side
of the second toe; the other three are inserted into the lateral sides of the
second, third, and fourth toes.
22.7.3
Discussion
22.7.3.1http://www.bartleby.com/107/131.html
22.7.4
Illustration
22.7.4.1http://www.bartleby.com/107/illus446.html
22.8 Category
22.8.1
Intrinsic
Foot (Plantar 4th Deep Layer)
23 DORSAL INTEROSSEI
(HAND)
23.1 Origin
23.1.1
Each from the 2 metacarpal bones
between which it inserts
23.2 Insertion
23.2.1
Bases of the proximal phalanges of
the 2nd, 3rd and 4th digits and the extensor expansion
23.3 Action
23.3.1
Abduct index, middle and ring
fingers from an axis through the middle finger
23.3.2
All assist in flexing the proximal
phalanges of the index, middle and ring fingers at the metacarpophalangeal
joints
23.3.3
Extending middle and distal
phalanges
23.4 Nerve Supply
23.4.1
Nerve
23.4.1.1Ulnar
(Deep Branch)
23.4.2
Roots
23.4.2.1C8
23.4.2.2T1
23.5 Synergists
23.5.1
Lumbricals
23.5.2
Palmar Interossei
23.5.3
Flexor Digitorum Profundus
23.5.4
Flexor Digitorum Superficialis
23.6 Category
23.6.1
Intrinsic Hand Intermediate (Midpalmar) (IHI)
24 EXTENSOR CARPI
RADIALIS BREVIS
24.1 Origin
24.1.1
Common extensor tendon from lateral
epicondyle of humerus
24.2 Insertion
24.2.1
Posterior surface of base of 3rd
metacarpal
24.3 Joints
24.3.1
Wrist
24.4 Action
24.4.1
Extension
24.4.2
Radial Deviation
24.5 Nerve Supply
24.5.1
Nerve
24.5.1.1Posterior
interosseous (deep radial)
24.5.2
Roots
24.5.2.1C7
24.5.2.2C8
24.6 Synergists
24.6.1
Extensor Carpi Radialis Longus
24.6.2
Extensor Carpi Ulnaris (Extension)
24.6.3
Extensor Carpi Radialis Longus
24.6.4
Flexor Carpi Radialis (Radial
Deviation)
24.7 Category
24.7.1
Wrist, Hand, and Fingers Posterior Extensors Deep (WHFPED)
25 EXTENSOR CARPI
RADIALIS LONGUS
25.1 Origin
25.1.1
Lower 1/3 of lateral supracondylar
ridge
25.1.2
Lateral epicondyle (few fibers from)
25.2 Insertion
25.2.1
Posterior surface of base of second
metacarpal
25.3 Joint
25.3.1
Wrist
25.4 Action
25.4.1
Extension
25.4.2
Radial Deviation
25.5 Nerve Supply
25.5.1
Nerve
25.5.1.1Radial
25.5.2
Roots
25.5.2.1C6
25.5.2.2C7
25.6 Synergists
25.6.1
Extensor Carpi Radialis Brevis
25.6.2
Extensor Carpi Ulnaris (Extension)
25.6.3
Flexor Carpi Radialis (Radial
Deviation)
25.7 Category
25.7.1
Wrist, Hand, and Fingers Posterior Extensors Superficial
(WHFPES)
26 EXTENSOR CARPI
ULNARIS
26.1 Origin
26.1.1
By two heads from lateral epicondyle
of humerus and middle 1/3 of posterior ridge of ulna
26.2 Insertion
26.2.1
Posterior surface of base of 5th
metacarpal
26.3 Joint
26.3.1
Wrist
26.4 Action
26.4.1
Extension
26.4.2
Ulnar Deviation
26.5 Nerve Supply
26.5.1
Nerve
26.5.1.1Posterior
interosseous (deep radial)
26.5.2
Roots
26.5.2.1C7
26.5.2.2C8
26.6 Synergists
26.6.1
Extensor Carpi Radialis Longus
26.6.2
Extensor Carpi Radialis Brevis
(Extension)
26.6.3
Flexor Carpi Ulnaris (Ulnar Deviation)
26.7 Category
26.7.1
Wrist, Hand, and Fingers Posterior Extensors Superficial
(WHFPES)
27 EXTENSOR DIGITI
MINIMI
27.1 Origin
27.1.1
The common tendon of the extensor
digitorum
27.2 Insertion
27.2.1
The tendon of the extensor digitorum
at the proximal phalanx of the little finger and into the dorsal expansion of
the finger extensor tendons
27.3 Joints
27.3.1
Metacarpophalangeal (MCP)
27.3.2
Interphalangeal (IP)
27.3.3
Wrist
27.4 Action
27.4.1
Extension (Proximal Phalanx Of The
Little Finger) (MCP)
27.4.2
Extension (Wrist)
27.4.3
Extension (Middle And Distal
Phalanges Especially When The Proximal Phalanx Is Held In Flexion) (IP)
27.5 Nerve Supply
27.5.1
27.5.1.1Posterior
interosseous (deep radial)
27.5.2
27.5.2.1C7
27.5.2.2C8
27.5.3
NOTE
27.5.3.1The
posterior interosseous nerve is a direct continuation of the deep radial nerve
after it has passed through the supinator .
27.6 Synergists
27.6.1
Extensor digitorum.
27.7 Category
27.7.1
28 EXTENSOR DIGITORUM
28.1 Origin
28.1.1
Common extensor tendon from lateral
epicondyle of humerus.
28.2 Insertion
28.2.1
By 4tendons, 1 to each finger, each
tendon dividing into 3 slips, the middle one attaching to the dorsal surface of
middle phalanx and the other 2 uniting to attach to dorsal surface of base of
distal phalanx.
28.3 Action
28.3.1
Extends phalanges at the
interphalangeal joints, con- tinued action extends the metacarpophalangeal and
car- pometacarpal articulations. Assists in extending wrist.
28.4 Nerve Supply
28.4.1
Posterior interosseous, (deep
radial) C7, 8.
28.5 Synergists
28.5.1
Extensor indicis, extensor digiti
minimi, lumbri- cales.
28.6 Category
28.6.1
29 EXTENSOR DIGITORUM
BREVIS
Back Table of Contents References
29.1 Word Derivation
and Pronunciation
29.2 Pronunciation
29.2.1.1Extensor Digitorum Brevis= eks-tenser, -sr brev is
is
29.2.1.2Pronunciation Key
29.2.2
Etymology
29.2.2.1Extensor=increases
angle at joint
29.2.2.2Digitorum=Finger
or Toe
29.2.2.3Brevis= Brief,
short
29.2.2.4Extensor= Latin
one who stretches, from ex-tendo, to stretch out
29.3 Attachments
29.3.1
Origin
29.3.1.1 Forepart
of the supralateral surface of the calcaneus
29.3.1.1.1
Distal and lateral surfaces of the
calcaneus
29.3.1.1.1.1
Distal part of superior and lateral
surfaces of calcaneus
29.3.1.2Lateral
talocalcaneal ligament
29.3.1.3Distal
to the groove for the peroneus brevis
29.3.1.4 Inferior
extensor retinaculum
29.3.1.4.1
Cruciate crural ligament
29.3.1.4.2
Apex
of the inferior extensor retinaculum
29.3.2
Insertion
29.3.2.1 Branches
into 3 tendons that insert into the lateral sides of the tendons of the
extensor digitorum longus of the 2nd, 3rd and 4th toes.
29.4 Joints
29.5Metatarsal/Tarsal
29.6Metatarsophalangeal
29.7Interphalangeal
29.8 Action
29.8.1
Extends the proximal phalanges of
the 2rid, 3rd and 4th toes
29.9 Nerve Supply
29.9.1
Nerve
29.9.1.1
Deep peroneal
29.9.2
Roots
29.9.2.1L4
29.9.2.2L5
29.9.2.3S1
29.9.2.4S2
29.10
Synergists
29.10.1 Extensor
digitorum longus
29.11
Muscle Tests
29.11.1 EXTENSOR DIGITORUM LONGUS
& BREVIS
29.12
Trigger Points
29.12.1
EXTENSOR DIGITORUM BREVIS
& EXTENSOR HALLUCIS BREVIS
29.13 Organ Reflexes
29.13.1 None
29.14
Acupressure/Acupuncture Theory
29.14.1 None
29.15
Nutritional
29.15.1 None
29.16
Discussion (Gray)
29.16.1 Extensor digitorum
brevis—The fascia on the dorsum of the foot is a thin membranous layer,
continuous above with the transverse and cruciate crural ligaments; on either
side it blends with the plantar aponeurosis; anteriorly it forms a sheath for
the tendons on the dorsum of the foot.
1
29.16.2 The Extensor
digitorum brevis (Fig. 441) is a broad, thin muscle, which arises from the
forepart of the upper and lateral surfaces of the calcaneus, in front of the
groove for the Peronæus brevis; from the lateral talocalcanean ligament; and
from the common limb of the cruciate crural ligament. It passes obliquely
across the dorsum of the foot, and ends in four tendons. The most medial, which
is the largest, is inserted into the dorsal surface of the base of the first
phalanx of the great toe, crossing the dorsalis pedis artery; it is frequently
described as a separate muscle—the Extensor hallucis brevis. The other three
are inserted into the lateral sides of the tendons of the Extensor digitorum
longus of the second, third, and fourth toes.
2
29.16.3 Variations.—Accessory
slips of origin from the talus and navicular, or from the external cunei-form
and third metatarsal bones to the second slip of the muscle, and one from the
cuboid to the third slip have been observed. The tendons vary in number and
position; they may be reduced to two, or one of them may be doubled, or an
additional slip may pass to the little toe. A supernumerary slip ending on one
of the metatarsophalangeal articulations, or joining a dorsal interosseous
muscle is not uncommon. Deep slips between this muscle and the Dorsal
interossei occur. 3
29.16.4 Nerves.—It is
supplied by the deep peroneal nerve. 4
29.16.5 Actions.—The
Extensor digitorum brevis extends the phalanges of the four toes into which it
is inserted, but in the great toe acts only on the first phalanx. The obliquity
of its direction counteracts the oblique movement given to the toes by the long
Extensor, so that when both muscles act, the toes are evenly extended.
29.16.6 Discussion
29.16.6.1 http://www.bartleby.com/107/131.html
29.16.7 Illustration
29.16.7.1 http://www.bartleby.com/107/illus441.html
29.17
Category
29.17.1 Intrinsic Foot (Dorsal
Muscles)
30 EXTENSOR DIGITORUM
LONGUS
Back Table of Contents References
30.1 Word Derivation
and Pronunciation
30.2 Pronunciation
30.2.1.1Extensor Digitorum Longus= eks-tenser, -sr
30.2.1.2Pronunciation Key
30.2.2
Etymology
30.2.2.1Extensor=increases
angle at joint
30.2.2.2Digitorum=Finger
or Toe
30.2.2.3Longus=Long
30.2.2.4Extensor= Latin one
who stretches, from ex-tendo, to stretch out
30.3 Attachments
30.3.1
Origin
30.3.1.1 Lateral
condyle of the tibia
30.3.1.2 Head
and proximal 3/4 of the anterior surface on the body of the fibula
30.3.1.3 Proximal
portion of the interosseus membrane
30.3.1.4 Deep
fascia
30.3.1.5 Adjacent
intermuscular septa
30.3.2
Insertion
30.3.2.1Divides into four
tendons after passing under the extensor retinaculum, to insert on to the
dorsal surfaces of the bases of the middle and distal phalanges of the 2nd -5th
toes
30.3.2.2Each tendon forms
an expansion on the dorsal surface of the toe, and divides into an intermediate
slip attached to the base of the middle phalanx and into two lateral slips
attached to base of the distal phalanx
30.4 Joints
30.5Ankle (Talocrural)
30.6Tibiofibular
(Distal)
30.7Metatarsal/Tarsal
30.8Metatarsophalangeal
30.9Interphalangeal
30.10
Action
30.10.1 Extends
the lateral 4 toes
30.10.1.1 Extends the
metatarsophalangeal joints and assists in extending the interphalangeal joints
of the 2nd through 5th digits.
30.10.2 Dorsiflexes
and everts foot at the ankle.
30.10.2.1 Assists in the
dorsiflexion of the ankle joint and eversion (Pronation) of the foot.
30.11
Nerve Supply
30.11.1 Nerve
30.11.1.1 Deep
peroneal
30.11.2
Roots
30.11.2.1 L4
30.11.2.2
L5
30.11.2.3
S1
30.12
Synergists
30.12.1 Extensor
digitorum brevis
30.13
Muscle Tests
30.13.1
EXTENSOR
DIGITORUM LONGUS & BREVIS
30.14
Trigger Points
30.14.1 Extensor Digitorum Hallucis
Longus
30.15 Organ Reflexes
30.15.1 None
30.16
Acupressure/Acupuncture Theory
30.16.1 None
30.17
Nutritional
30.17.1 None
30.18
Discussion (Gray)
30.18.1 The Extensor
digitorum longus is a penniform muscle, situated at the lateral part of the
front of the leg. It arises from the lateral condyle of the tibia; from the
upper three-fourths of the anterior surface of the body of the fibula; from the
upper part of the interosseous membrane; from the deep surface of the fascia;
and from the intermuscular septa between it and the Tibialis anterior on the medial,
and the Peronæi on the lateral side. Between it and the Tibialis anterior are
the upper portions of the anterior tibial vessels and deep peroneal nerve. The
tendon passes under the transverse and cruciate crural ligaments in company
with the Peronæus tertius, and divides into four slips, which run forward on
the dorsum of the foot, and are inserted into the second and third phalanges of
the four lesser toes. The tendons to the second, third, and fourth toes are
each joined, opposite the metatarsophalangeal articulation, on the lateral side
by a tendon of the Extensor digitorum brevis. The tendons are inserted in the
following manner: each receives a fibrous expansion from the Interossei and
Lumbricalis, and then spreads out into a broad aponeurosis, which covers the
dorsal surface of the first phalanx: this aponeurosis, at the articulation of
the first with the second phalanx, divides into three slips—an intermediate,
which is inserted into the base of the second phalanx; and two collateral
slips, which, after uniting on the dorsal surface of the second phalanx, are
continued onward, to be inserted into the base of the third phalanx. 7
30.18.2 Variations.—This
muscle varies considerably in the modes of origin and the arrangement of its
various tendons. The tendons to the second and fifth toes may be found doubled,
or extra slips are given off from one or more tendons to their corresponding
metatarsal bones, or to the short extensor, or to one of the interosseous
muscles. A slip to the great toe from the innermost tendon has been found.
30.18.3 Discussion
30.18.3.1 http://www.bartleby.com/107/129.html
30.18.4 Illustration
30.18.4.1 http://www.bartleby.com/107/illus437.html
30.18.4.2 http://www.bartleby.com/107/illus440.html
30.19
Category
30.19.1 Foot & Toes (Anterior
Compartment)
31 EXTENSOR HALLUCIS
BREVIS
Back Table of Contents References
31.1 Word Derivation
and Pronunciation
31.2 Pronunciation
31.2.1.1Extensor Hallucis
Brevis
31.2.1.1.1 Extensor=ik-'sten(t)-s&r
31.2.1.1.2
Hallux=ha-l&ks
31.2.1.1.3
Halluces= 'ha-l&-"sEz,
'hal-y&-/
31.2.1.2Pronunciation Key
31.2.2
Etymology
31.2.2.1Extensor=increases
angle at joint
31.2.2.2Hallucis=Hallux or
great toe
31.2.2.2.1
New
Latin, from Latin hallus, hallux
: the innermost digit (as the
big toe) of a hind or lower limb
31.2.2.3Brevis= Short or
Brief
31.3 Attachments
31.3.1
Origin
31.3.1.1Calcaneus
(Forepart medial aspect)
31.3.1.1.1
Anterior superior medial aspect of
calcaneus
31.3.1.1.2
Distal part of superior and
relatively lateral surfaces of calcaneus
31.3.1.2Lateral
talocalcaneal ligament
31.3.1.3 Inferior
extensor retinaculum
31.3.1.3.1
Cruciate
crural ligament
31.3.1.3.2
Apex
of the inferior extensor retinaculum
31.3.2
Insertion
31.3.2.1Dorsal
surface of the base of proximal phalanx of hallux
31.4 Joints
31.51st
Metatarsal/Tarsal
31.61st
Metatarsophalangeal
31.7 Action
31.7.1
Extends proximal phalanx of hallux
(big toe).
31.7.1.1Extends
the metatarsophalangeal joint of the great toe
31.7.1.2The extensor hallucis
brevis is the medial section (Slip) of the extensor digitorum brevis, which
extends the proximal phalanges of the 2nd- 4th toes.
31.8 Nerve Supply
31.8.1
Nerve
31.8.1.1Deep
peroneal
31.8.2
Roots
31.8.2.1L4
31.8.2.2L5
31.8.2.3S1
31.8.2.4S2
31.9 Synergists
31.9.1
Extensor hallucis longus
31.10
Muscle Tests
31.10.1
EXTENSOR
HALLUCIS LONGUS & BREVIS
31.11
Trigger Points
31.11.1 EXTENSOR DIGITORUM BREVIS
& EXTENSOR HALLUCIS BREVIS
31.12 Organ Reflexes
31.12.1 None
31.12.2 Illustrations
31.13
Acupressure/Acupuncture Theory
31.13.1 None
31.14
Nutritional
31.14.1 None
31.15
Discussion (Gray)
31.15.1 Extensor digitorum
brevis—The fascia on the dorsum of the foot is a thin membranous layer,
continuous above with the transverse and cruciate crural ligaments; on either side
it blends with the plantar aponeurosis; anteriorly it forms a sheath for the
tendons on the dorsum of the foot. 1
31.15.2 The Extensor
digitorum brevis (Fig. 441) is a broad, thin muscle, which arises from the
forepart of the upper and lateral surfaces of the calcaneus, in front of the
groove for the Peronæus brevis; from the lateral talocalcanean ligament; and
from the common limb of the cruciate crural ligament. It passes obliquely
across the dorsum of the foot, and ends in four tendons. The most medial, which
is the largest, is inserted into the dorsal surface of the base of the first
phalanx of the great toe, crossing the dorsalis pedis artery; it is frequently
described as a separate muscle—the Extensor hallucis brevis. The other three
are inserted into the lateral sides of the tendons of the Extensor digitorum
longus of the second, third, and fourth toes.
2
31.15.3 Variations.—Accessory
slips of origin from the talus and navicular, or from the external cunei-form
and third metatarsal bones to the second slip of the muscle, and one from the
cuboid to the third slip have been observed. The tendons vary in number and
position; they may be reduced to two, or one of them may be doubled, or an
additional slip may pass to the little toe. A supernumerary slip ending on one
of the metatarsophalangeal articulations, or joining a dorsal interosseous
muscle is not uncommon. Deep slips between this muscle and the Dorsal
interossei occur. 3
31.15.4 Nerves.—It is
supplied by the deep peroneal nerve. 4
31.15.5 Actions.—The
Extensor digitorum brevis extends the phalanges of the four toes into which it
is inserted, but in the great toe acts only on the first phalanx. The obliquity
of its direction counteracts the oblique movement given to the toes by the long
Extensor, so that when both muscles act, the toes are evenly extended.
31.15.6 Discussion
31.15.6.1 http://www.bartleby.com/107/131.html
31.15.7 Illustration
31.15.7.1 http://www.bartleby.com/107/illus441.html
31.16
Category
31.16.1 Intrinsic Foot (Dorsal
Muscles)
31.17
Note
31.17.1 (Note:
The extensor hallucis brevis is the medial section of the extensor
digitorum brevis.)
32 EXTENSOR HALLUCIS
LONGUS
Back Table of Contents References
32.1 Word Derivation
and Pronunciation
32.2 Pronunciation
32.2.1.1Extensor Hallucis
Longus
32.2.1.1.1 Extensor=ik-'sten(t)-s&r
32.2.1.1.2
Hallux=ha-l&ks
32.2.1.1.3
Halluces= 'ha-l&-"sEz,
'hal-y&-/
32.2.1.2Pronunciation Key
32.2.2
Etymology
32.2.2.1Extensor=increases
angle at joint
32.2.2.2Hallucis=Hallux or
great toe
32.2.2.2.1
New
Latin, from Latin hallus, hallux
: the innermost digit (as the
big toe) of a hind or lower limb
32.2.2.3Longus= long
32.3 Attachments
32.3.1
Origin
32.3.1.1 Middle
1/2 ( 2/4) of the anterior surface of the fibula
32.3.1.2 Adjacent
interosseous membrane
32.3.2
Insertion
32.3.2.1 Dorsal
surface of base of distal phalanx of hallux (big toe)
32.4 Joints
32.5Ankle (Talocrural)
32.6Tibiofibular
(Distal)
32.71st
Metatarsal/Tarsal
32.81st
Metatarsophalangeal
32.91st Interphalangeal
32.10
Action
32.10.1 Extends
the distal phalanx of the big toe.
32.10.2 Continued
action extends proximal phalanx
32.10.2.1 Metatarsophalangeal
and interphalangeal joints
32.10.3 Dorsiflexes
and inverts (Supinates) the foot at the ankle.
32.11
Nerve Supply
32.11.1 Nerve
32.11.1.1 Deep
peroneal
32.11.2
Roots
32.11.2.1 L4
32.11.2.2 L5
32.11.2.3 S1
32.12
Synergists
32.12.1 Extensor
Hallucis Brevis
32.13
Muscle Tests
32.13.1 EXTENSOR HALLUCIS LONGUS
& BREVIS
32.14
Trigger Points
32.14.1
EXTENSOR DIGITORUM LONGUS
& EXTENSOR HALLUCIS LONGUS
32.15 Organ Reflexes
32.15.1 None
32.15.2 Illustrations
32.16
Acupressure/Acupuncture Theory
32.16.1 None
32.17
Nutritional
32.17.1 None
32.18
Discussion (Gray)
32.18.1 The Extensor
hallucis longus (Extensor proprius hallucis) is a thin muscle, situated between
the Tibialis anterior and the Extensor digitorum longus. It arises from the
anterior surface of the fibula for about the middle two-fourths of its extent,
medial to the origin of the Extensor digitorum longus; it also arises from the
interosseous membrane to a similar extent. The anterior tibial vessels and deep
peroneal nerve lie between it and the Tibialis anterior. The fibers pass
downward, and end in a tendon, which occupies the anterior border of the
muscle, passes through a distinct compartment in the cruciate crural ligament,
crosses from the lateral to the medial side of the anterior tibial vessels near
the bend of the ankle, and is inserted into the base of the distal phalanx of
the great toe. Opposite the metatarsophalangeal articulation, the tendon gives
off a thin prolongation on either side, to cover the surface of the joint. An
expansion from the medial side of the tendon is usually inserted into the base
of the proximal phalanx. 5
32.18.2
32.18.3 Variations.—Occasionally
united at its origin with the Extensor digitorum longus. Extensor ossis
metatarsi hallucis, a small muscle, sometimes found as a slip from the Extensor
hallucis longus, or from the Tibialis anterior, or from the Extensor digitorum
longus, or as a distinct muscle; it traverses the same compartment of the transverse
ligament with the Extensor hallucis longus.
32.18.4 Discussion
32.18.4.1 http://www.bartleby.com/107/129.html
32.18.5 Illustration
32.18.5.1 http://www.bartleby.com/107/illus437.html
32.18.5.2 http://www.bartleby.com/107/illus440.html
32.19
Category
32.19.1 Foot & Toes (Anterior
Compartment)
33 EXTENSOR INDICIS
33.1 Origin
33.1.1
Dorsal surface of distal half of
ulna.
33.2 Insertion
33.2.1
Index finger extensor digitorum
tendon.
33.3 Action
33.3.1
Extension of all phalanges of index
finger. Assists in wrist extension.
33.4 Nerve Supply
33.4.1
Posterior Interosseous, (deep
radial), C7,8.
33.5 Synergists
33.5.1
Extensor digitorum.
33.6 Category
33.6.1
34 EXTENSOR POLLICIS
BREVIS
34.1 Origin
34.1.1
The posterior surface of the distal
end of the body of the ulna near the middle and the adjacent interosseous
membrane.
34.2 Insertion
34.2.1
The posterior surface of the base of
the proximal phalanx of the thumb.
34.3 Action
34.3.1
Extends the proximal phalanx of the
thumb. Continued action extends and assists abduction of the 1 st metacarpal.
34.4 Nerve Supply
34.4.1
Posterior interosseous nerve (deep
radial nerve), C6,7.
34.5 Synergists
34.5.1
Abductor pollicis longus, extensor
pollicis longus.
34.6 Category
34.6.1
35 EXTENSOR POLLICIS
LONGUS
35.1 Origin
35.1.1
Posterior surface of the middle 1/3
of the ulna and the interosseous membrane.
35.2 Insertion
35.2.1
The posterior surface of the base of
the distal phalanx of the thumb.
35.3 Action
35.3.1
Extends the distal phalanx of the
thumb. Continued action, extends proximal phalanx and metacarpal, and adducts
the 1st metacarpal.
35.4 Nerve Supply
35.4.1
Posterior interosseous nerve (deep
radial nerve) C7,8.
35.5 Synergists
35.5.1
Extensor pollicis brevis.
35.6 Category
35.6.1
36 EXTERNAL ABDOMINAL
OBLIQUE=ANT DIV
36.1 Origin
36.1.1
External surfaces and inferior
borders of the Sth -12th ribs by tendinous slips that interdigitate with those
of serratus anterior and latissimus dorsi.
36.2 Insertion
36.2.1
Linea alba by means of the broad
abdominal aponeurosis from ribs to crest of pubis, inquinalligament and the
anterior half of the iliac crest along the outer lip.
36.3 Action
36.3.1
Acting unilaterally, rotates the
trunk to the opposite side, and flexes it laterally on the side of muscle
contraction. If rotation is only activity, the opposite internal oblique is synergist.
Acting bilaterally, flexes the trunk anteriorly, supports and compresses the
abdominal viscera, giving anterior support to the spinal column. Gives anterior
stabilization to pelvis, decreasing lordosis. Assists in forced expiration.
36.4 Nerve Supply
36.4.1
Branches of the 7th .12th
intercostal nerves.
36.5 Synergists
36.5.1
Rectus abdominis, internal oblique
and external oblique abdominals of opposite side. Psoas on lumbar spine in
total trunk flexion.
36.6 Category
36.6.1
37 EXTERNAL ABDOMINAL
OBLIQUE=LAT DIV
37.1 Origin
37.1.1
37.2 Insertion
37.2.1
37.3 Action
37.3.1
37.4 Nerve Supply
37.4.1
37.5 Synergists
37.5.1
37.6 Category
37.6.1
38 EXTERNAL ANAL
SPHINCTER
38.1 Origin
38.1.1
38.2 Insertion
38.2.1
38.3 Action
38.3.1
38.4 Nerve Supply
38.4.1
38.5 Synergists
38.5.1
38.6 Category
38.6.1
39 EXTERNAL
INTERCOSTALS
39.1 Origin
39.1.1
Inferior border of rib above.
39.2 Insertion
39.2.1
Superior border of rib below
39.3 Action
39.3.1
Elevate ribs during inspiration.
39.4 Nerve Supply
39.4.1
Branches from corresponding
intercostal nerves.
39.5 Synergists
39.5.1
Serratus posterior superior,
levatores costarum. Scaleni group.
39.6 Category
39.6.1
40 EXTRINSIC
AURICULAR MUSCLES
40.1 Origin
40.1.1
Auriculari~
anterior: Lateral edge of the epicranial aponeurosis.
40.1.2
Auricularis
superior: EQicranial aponeurosis. Auricularis posterior: Mastoid part of the
temporal bone.
40.2 Insertion
40.2.1
Auricularis
anterior: The spine of the helix.
40.2.2
Auricularis
superior: The upper part of the cranial surface of the auricle.
40.2.3
Auricularis
posterior: By two or three fasciculi into the ponticulus on the eminentia
conchae.
40.3 Action
40.3.1
Minimal
action in man.
40.3.2
Auricularis
anterior: Draws auricle forwards and up.
40.3.3
Auricularis
superior: Elevates the auricle.
40.3.4
Auricularis
posterior: Draws the auricle back.
40.4 Nerve Supply
40.4.1
Auricularis
anterior and superior: Temporal bral}ches 9f the fa~ial nerve (VII).
40.4.2
AuriCularis
posterior: PosterIor aurIcular branch of the facial nerve (VII).
40.5 Arterial supply
40.5.1
Auricular
rami from the posterior auricular branch of the external carotid artery, the
anterior auricular branches of the superficial temporal artery, and the
auricular branch of the occipital artery.
40.6 Synergists
40.6.1
Frontalis
and occipitalis, indirectly.
40.7 Antagonist
40.7.1
None
40.8 Category
40.8.1
41 FLEXOR CARPI
RADIALIS
41.1 Origin
41.1.1
Common flexor tendon from medial
epicondyle of humerus.
41.2 Insertion
41.2.1
Anterior surfaces of bases of 2nd
and 3rd metacar- pals.
41.3 Action
41.3.1
Flexes and radially deviates the
hand at the wrist.
41.4 Nerve Supply
41.4.1
Median nerve, C6, 7.
41.5 Synergists
41.5.1
Flexor carpi ulnaris and palmaris
longus for flexion. Extension carpi radialis longus and brevis for radial
deviation.
41.6 Category
41.6.1
42 FLEXOR CARPI
ULNARIS
42.1 Origin
42.1.1
By 2 heads from medial epicondyle of
humerus and medial border of olecranon process of ulna.
42.2 Insertion
42.2.1
Palmar surface of pisiform and
hamate carpal bones and base of Sth metacarpal.
42.3 Action
42.3.1
Flexes and ulnarly deviates the hand
at the wrist.
42.4 Nerve Supply
42.4.1
Ulnar, C7, 8.
42.5 Synergists
42.5.1
Flexor carpi radials and palmaris
longus for flexion. Extensor carpi ulnaris for ulnar deviation.
42.6 Category
42.6.1
43 FLEXOR DIGITI
MINIMI BREVIS (FOOT)
Back Table of Contents References
43.1 Attachments
43.1.1
Origin
43.1.1.1 Base
of the 5th metatarsal bone
43.1.2
Insertion
43.1.2.1 Lateral
side of the base of the proximal phalanx of the little toe
43.2 Action
43.2.1
Flexes the proximal phalanx of the
5th toe.
43.3 Nerve Supply
43.3.1
Nerve
43.3.1.1Lateral
plantar nerve
43.3.2
Roots
43.3.2.1S2
43.3.2.2S3
43.4 Synergists
43.4.1
Flexor digitorum brevis
43.4.2
Flexor digitorum longus
43.4.3
Quadratus plantae
43.5 Muscle
Tests
43.5.1
43.6 Trigger Points
43.6.1
43.7 Discussion (Gray)
43.7.1
The Flexor digiti quinti brevis (Flexor brevis minimi
digiti) lies under the metatarsal bone of the little toe, and resembles one of
the Interossei. It arises from the base of the fifth metatarsal bone, and from
the sheath of the Peronæus longus; its tendon is inserted into the lateral side
of the base of the first phalanx of the fifth toe. Occasionally a few of the
deeper fibers are inserted into the lateral part of the distal half of the
fifth metatarsal bone; these are described by some as a distinct muscle, the
Opponens digiti quinti.
43.7.2
Discussion
43.7.2.1http://www.bartleby.com/107/131.html
43.7.3
Illustration
43.7.3.1http://www.bartleby.com/107/illus445.html
43.8 Category
43.8.1
Intrinsic
Foot (Plantar 3rd Layer)
44 FLEXOR DIGITI
MINIMI BREVIS (HAND)
44.1 Origin
44.1.1
Hamulus or hook of the hamate bone
and flexor retinaculum.
44.2 Insertion
44.2.1
Ulnar side of the base of the
proximal phalanx of the Sth finger.
44.3 Action
44.3.1
Flexes the Sth digit at the
metacarpophalangeal articula- tion.
44.4 Nerve Supply
44.4.1
Deep branch of ulnar nerve, C8, T1.
44.5 Synergists
44.5.1
Flexor digitorum superficialis,
flexor digitorum profundus, opponens digiti minimi, interossei.
44.6 Category
44.6.1
45 FLEXOR DIGITORUM
BREVIS
Back Table of Contents References
45.1 Attachments
45.1.1
Origin
45.1.1.1Medial
process of tuberosity of the calcaneus
45.1.1.2Central
part of the plantar aponeurosis (The entire muscle belly is firmly united with
the plantar aponeurosis)
45.1.1.3 Intermuscular
septa
45.1.2
Insertion
45.1.2.1Divides
into 4 tendons that insert into the middle phalanges of the 2nd -5th toes
45.2 Action
45.2.1
Plantar flexes the middle phalanges
on the proximal phalanges
45.2.2
Continued action flexes the proximal
phalanges on the metatarsals.
45.3 Nerve Supply
45.3.1
Nerve
45.3.1.1Medial Plantar (Tibial)
45.3.2
Roots
45.3.2.1L4
45.3.2.2L5
45.3.2.3S1
45.3.2.4S2
45.3.2.5S3
45.4 Synergists
45.4.1
Flexor digitorum longus
45.5 Muscle
Tests
45.5.1
45.6 Trigger Points
45.6.1
45.7 Discussion (Gray)
45.7.1
The Flexor digitorum brevis lies in the middle of the sole
of the foot, immediately above the central part of the plantar aponeurosis, with
which it is firmly united. Its deep surface is separated from the lateral
plantar vessels and nerves by a thin layer of fascia. It arises by a narrow
tendon, from the medial process of the tuberosity of the calcaneus, from the
central part of the plantar aponeurosis, and from the intermuscular septa
between it and the adjacent muscles. It passes forward, and divides into four
tendons, one for each of the four lesser toes. Opposite the bases of the first
phalanges, each tendon divides into two slips, to allow of the passage of the
corresponding tendon of the Flexor digitorum longus; the two portions of the
tendon then unite and form a grooved channel for the reception of the
accompanying long Flexor tendon. Finally, it divides a second time, and is inserted
into the sides of the second phalanx about its middle. The mode of division of
the tendons of the Flexor digitorum brevis, and of their insertion into the
phalanges, is analogous to that of the tendons of the Flexor digitorum sublimis
in the hand. 14
45.7.2
Variations.—Slip to the little toe frequently wanting, 23
per cent.; or it may be replaced by a small fusiform muscle arising from the
long flexor tendon or from the Quadratus plantæ. 15
45.7.3
Fibrous Sheaths of the Flexor Tendons.—The terminal portions
of the tendons of the long and short Flexor muscles are contained in
osseoaponeurotic canals similar in their arrangement to those in the fingers.
These canals are formed above by the phalanges and below by fibrous bands,
which arch across the tendons, and are attached on either side to the margins
of the phalanges. Opposite the bodies of the proximal and second phalanges the
fibrous bands are strong, and the fibers are transverse; but opposite the
joints they are much thinner, and the fibers are directed obliquely. Each canal
contains a mucous sheath, which is reflected on the contained tendons.
45.7.4
Discussion
45.7.4.1http://www.bartleby.com/107/131.html
45.7.5
Illustration
45.7.5.1http://www.bartleby.com/107/illus443.html
45.8 Category
45.8.1
Intrinsic
Foot Plantar First Superficial Layer (IFP1)
46 FLEXOR DIGITORUM
LONGUS
Back Table of Contents References
46.1 Word Derivation
and Pronunciation
46.2 Pronunciation
46.2.1.1Flexor Digitorum
Longus
46.2.1.1.1
Flexor=flek-s&r,
-"sor
46.2.1.2Pronunciation Key
46.2.2
Etymology
46.2.2.1Flexor=decreases
angle at joint
46.2.2.2Digitorum=Finger
or Toe
46.2.2.3Longus= Long
46.3 Attachments
46.3.1
Origin
46.3.1.1Posterior
surface of middle 3/5th of tibia
46.3.1.2Posterior
Tibialis Fascia
46.3.2
Insertion
46.3.2.1Divides
into 4 tendons that insert on the plantar surfaces of bases of distal phalanges
of the 2nd -5th toes
46.4 Joints
46.5Ankle (Talocrural)
46.6Tibiofibular
(Distal)
46.7Metatarsal/Tarsal
46.8Metatarsophalangeal
46.9Interphalangeal
46.10
Action
46.10.1 Flexes
proximal and distal phalanges at all interphalangeal and metatarsophalangeal
articulations of 2nd -5th toes.
46.10.2 Plantar
flexion (Foot-Ankle)
46.10.3 Inversion
(Foot-Ankle)
46.10.4 Medial
ankle stabilization
46.11
Nerve Supply
46.11.1 Nerve
46.11.1.1 Tibial
46.11.2 Roots
46.11.2.1 L5
46.11.2.2 S1
46.11.2.3 S2
46.11.2.4 S3
46.12
Synergists
46.12.1 Tibialis
Posterior
46.12.2 Flexor
Hallucis Longus
46.12.3 Flexor
Digitorum Brevis
46.13
Muscle Tests
46.13.1
FLEXOR
DIGITORUM LONGUS & QUADRATUS PLANTAE
46.14
Trigger Points
46.14.1 FLEXOR DIGITORUM LONGUS &
FLEXOR HALLUCIS LONGUS
46.15 Organ Reflexes
46.15.1 None
46.15.2 Illustrations
46.16
Acupressure/Acupuncture Theory
46.16.1 None
46.17
Nutritional
46.17.1 None
46.18
Discussion (Gray)
46.18.1 The Flexor
digitorum longus is situated on the tibial side of the leg. At its origin it is
thin and pointed, but it gradually increases in size as it descends. It arises
from the posterior surface of the body of the tibia, from immediately below the
popliteal line to within 7 or 8 cm. of its lower extremity, medial to the
tibial origin of the Tibialis posterior; it also arises from the fascia
covering the Tibialis posterior. The fibers end in a tendon, which runs nearly
the whole length of the posterior surface of the muscle. This tendon passes
behind the medial malleolus, in a groove, common to it and the Tibialis
posterior, but separated from the latter by a fibrous septum, each tendon being
contained in a special compartment lined by a separate mucous sheath. It passes
obliquely forward and lateralward, superficial to the deltoid ligament of the
ankle-joint, into the sole of the foot (Fig. 444), where it crosses below the
tendon of the Flexor hallucis longus, and receives from it a strong tendinous
slip. It then expands and is joined by the Quadratus plantæ, and finally
divides into four tendons, which are inserted into the bases of the last
phalanges of the second, third, fourth, and fifth toes, each tendon passing through
an opening in the corresponding tendon of the Flexor digitorum brevis opposite
the base of the first phalanx. 27
46.18.2
46.18.3 Variations.—Flexor
accessorius longus digitorum, not infrequent, origin from fibula, or tibia, or
the deep fascia and ending in a tendon which, after passing beneath the
laciniate ligament, joins the tendon of the long flexor or the Quadratus
plantæ.
46.18.4 Discussion
46.18.4.1 http://www.bartleby.com/107/129.html
46.18.5 Illustration
46.18.5.1 http://www.bartleby.com/107/illus439.html
46.18.5.2 http://www.bartleby.com/107/illus440.html
46.19
Category
46.19.1 Foot & Toes (Posterior
Deep Compartment)
46.20
Individual Muscle Illustration
46.20.1 Posterior
and Plantar View
47 FLEXOR DIGITORUM
PROFUNDUS
47.1 Origin
47.1.1
Upper :}f4 of the anterior
and medial surfaces of the ulna, interosseous membrane and deep fascia of the
forearm.
47.2 Insertion
47.2.1
4 tendons (1 to each finger) to
palmar surface of base of distal phalanx, after passing through tendon of
flexor digitorum superficialis.
47.3 Action
47.3.1
A exes the distal phalanges of the
four fingers. Assists in flexing metacarpophalangeal, carpometacapal and wrist
joints.
47.4 Nerve Supply
47.4.1
Nerve to portion of muscle which
correlates with index and middle fingers, anterior interosseous branch of the
median, C8, T1 ; nerve to portion of muscle which correlates with ring and
little fingers, ulnar, C8, T1.
47.5 Synergists
47.5.1
Aexor digitorum superficialis.
47.6 Category
47.6.1
47.7 View
47.7.1
Anterior View
48 FLEXOR DIGITORUM
SUPERFICIALIS
48.1 Origin
48.1.1
HUMERO-ULNAR HEAD: Medial epicondyle
of the humerus by the common flexor tendon, ulnar collateral ligament of the
elbow and the coronoid process of ulna.
48.1.2
RADIAL: Oblique line of the radius
extending from the radial tuberosity to the insertion of the pronator teres.
48.2 Insertion
48.2.1
4 tendons (1 for each finger) divide
for the passage of the tendons of flexor digitorum profundus then insert as 2
slips on the sides of the shaft of the middle phalanx.
48.3 Action
48.3.1
Flexes the phalanx of each finger on
the proximal phalanx. Continued action, flexes the proximal phalanx at the
hand, flexes the hand at the wrist.
48.4 Nerve Supply
48.4.1
Median C7, 8, T1.
48.5 Synergists
48.5.1
Flexor digitorum profundus.
48.6 Category
48.6.1
48.7 View
48.7.1
- Anterior View
49 FLEXOR HALLUCIS
BREVIS
Back Table of Contents References
49.1 Attachments
49.1.1
Origin
49.1.1.1 Medial
portion of the plantar surface of the cuboid bone
49.1.1.2 Adjacent
portion of the lateral cuneiform bone
49.1.1.3 Prolongation
of the tendon of the tibialis posterior
49.1.2
Insertion
49.1.2.1 Medial
and lateral sides of base of proximal phalanx of the big toe
49.2 Action
49.2.1
Flexes metatarsophalangeal
articulation of big toe
49.3 Nerve Supply
49.3.1
Nerve
49.3.1.1Medial
plantar
49.3.2
Roots
49.3.2.1L4
49.3.2.2L5
49.3.2.3S1
49.3.2.4S2
49.3.2.5S3
49.4 Synergists
49.4.1
Flexor hallucis longus
49.5 Muscle
Tests
49.5.1
49.6 Trigger Points
49.6.1
49.7 Discussion (Gray)
49.7.1
The Flexor hallucis brevis arises, by a pointed tendinous
process, from the medial part of the under surface of the cuboid bone, from the
contiguous portion of the third cuneiform, and from the prolongation of the
tendon of the Tibialis posterior which is attached to that bone. It divides in
front into two portions, which are inserted into the medial and lateral sides
of the base of the first phalanx of the great toe, a sesamoid bone being
present in each tendon at its insertion. The medial portion is blended with the
Abductor hallucis previous to its insertion; the lateral portion with the
Adductor hallucis; the tendon of the Flexor hallucis longus lies in a groove
between them; the lateral portion is sometimes described as the first
Interosseous plantaris. 23
49.7.2
Variations.—Origin subject to considerable variation; it
often receives fibers from the calcaneus or long plantar ligament. Attachment
to the cuboid sometimes wanting. Slip to first phalanx of the second toe.
49.7.3
Discussion
49.7.3.1http://www.bartleby.com/107/131.html
49.7.4
Illustration
49.7.4.1http://www.bartleby.com/107/illus445.html
49.8 Category
49.8.1
Intrinsic
Foot (Plantar 3rd Layer)
49.9 View
49.9.1
Plantar View (3rd Plantar Layer)
50 FLEXOR HALLUCIS
LONGUS
Back Table of Contents References
50.1 Word Derivation
and Pronunciation
50.2 Pronunciation
50.2.1.1Flexor Hallucis
Brevis
50.2.1.1.1
Flexor=flek-s&r,
-"sor
50.2.1.1.2
Hallux=ha-l&ks
50.2.1.1.3
Halluces= 'ha-l&-"sEz,
'hal-y&-/
50.2.1.2Pronunciation Key
50.2.2
Etymology
50.2.2.1Flexor=decreases
angle at joint
50.2.2.2Hallucis=Hallux or
great toe
50.2.2.2.1
New
Latin, from Latin hallus, hallux
: the innermost digit (as the
big toe) of a hind or lower limb
50.2.2.3Longus= long
50.3 Attachments
50.3.1
Origin
50.3.1.1Distal
(Lower) 2l3 of posterior surface of fibula
50.3.1.2Interosseous
membrane
50.3.1.3Adjacent
intermuscular septa and fascia
50.3.2
Insertion
50.3.2.1Plantar
surface of the base of distal phalanx of the hallux (big (great) toe)
50.3.3
Note
50.3.3.1The flexor
hallucis longus is connected to the flexor digitorum longus by a strong
tendinous slip
50.4 Joints
50.5Ankle (Talocrural)
50.6Tibiofibular
(Distal)
50.71st
Metatarsal/Tarsal
50.81st
Metatarsophalangeal
50.91st
Interphalangeal
50.10
Action
50.10.1 Flexion
(big toe)
50.10.1.1 Flexes the
interphalangeal joint of the great toe
50.10.1.2 Assists in the flexion
of the metatarsophalangeal joint
50.10.2 Plantar
flexion (Foot-Ankle)
50.10.2.1 Continued action
aids in plantar flexing the foot
50.10.3 Inversion
(Foot-Ankle)
50.10.4 Medial
ankle stabilization
50.11
Nerve Supply
50.11.1 Nerve
50.11.1.1 Tibial
50.11.2 Roots
50.11.2.1 L5
50.11.2.2 S1
50.11.2.3 S2
50.11.2.4 S3
50.12
Synergists
50.12.1 Flexor
Hallucis Brevis
50.13
Muscle Tests
50.13.1 FLEXOR HALLUCIS LONGUS
50.14
Trigger Points
50.14.1
FLEXOR DIGITORUM LONGUS &
FLEXOR HALLUCIS LONGUS
50.15 Organ Reflexes
50.15.1
Sex Glands
50.15.2 Illustrations
50.16
Acupressure/Acupuncture Theory
50.16.1 Organs
50.16.1.1 Pericardium and Triple Burner
50.16.2 Channels
Discussion
50.16.2.1 Pericardium (Circulation Sex)
50.16.3 Channel
50.16.3.1 Pericardium (Circulation Sex)
Illustration
50.16.4 Command Points
50.16.4.1 Pericardium (Circulation Sex)
50.17
Nutritional
50.17.1 Raw bone
concentrate correlating with tarsal tunnel syndrome or other subluxations of
the foot.
50.18
Discussion (Gray)
50.18.1 The Flexor
hallucis longus is situated on the fibular side of the leg. It arises from the
inferior two-thirds of the posterior surface of the body of the fibula, with
the exception of 2.5 cm. at its lowest part; from the lower part of the
interosseous membrane; from an intermuscular septum between it and the Peronæi,
laterally, and from the fascia covering the Tibialis posterior, medially. The
fibers pass obliquely downward and backward, and end in a tendon which occupies
nearly the whole length of the posterior surface of the muscle. This tendon
lies in a groove which crosses the posterior surface of the lower end of the
tibia, the posterior surface of the talus, and the under surface of the
sustentaculum tali of the calcaneus; in the sole of the foot it runs forward
between the two heads of the Flexor hallucis brevis, and is inserted into the
base of the last phalanx of the great toe. The grooves on the talus and
calcaneus, which contain the tendon of the muscle, are converted by tendinous
fibers into distinct canals, lined by a mucous sheath. As the tendon passes
forward in the sole of the foot, it is situated above, and crosses from the
lateral to the medial side of the tendon of the Flexor digitorum longus, to
which it is connected by a fibrous slip.
25
50.18.2 Variations.—Usually
a slip runs to the Flexor digitorum and frequently an additional slip runs from
the Flexor digitorum to the Flexor hallucis. Peroneocalcaneus internus, rare,
origin below or outside the Flexor hallucis from the back of the fibula, passes
over the sustentaculum tali with the Flexor hallucis and is inserted into the
calcaneum.
50.18.3 Discussion
50.18.3.1 http://www.bartleby.com/107/129.html
50.18.4 Illustration
50.18.4.1 http://www.bartleby.com/107/illus439.html
50.18.4.2 http://www.bartleby.com/107/illus440.html
50.19
Category
50.19.1 Foot & Toes (Posterior
Deep Compartment)
50.20
View
50.20.1
Posterior and Plantar View
51 FLEXOR POLLICIS
BREVIS
51.1 Origin
51.1.1
SUPERFICIAL HEAD: Distal border of
the flexor retinaculum and tubercle of the trapezium bone.
51.1.2
DEEP HEAD: Trapezoid and capitate
bones.
51.2 Insertion
51.2.1
Radial side of the base of the
proximal phalanx of the thumb.
51.3 Action
51.3.1
Flexes proximal phalanx of the
thumb. Continued action, flexes the 1st metacarpal and rotates it medially.
51.4 Nerve Supply
51.4.1
SUPERFICIAL HEAD: Median, C6, 7;
mostly cs and T1.
51.4.2
DEEP HEAD: Ulnar, C8, T1.
51.5 Synergists
51.5.1
Flexor pollicis longus, adductor
pollicis.
51.6 Category
51.6.1
51.7 View
51.7.1
Anterior View
52 FLEXOR POLLICIS
LONGUS
52.1 Origin
52.1.1
Anterior surface of middle 1/2 of
radius. Adjacent interos- seous membrane and a slip from the coronoid process
of the ulna or medial epicondyle of humerus.
52.2 Insertion
52.2.1
Palmar surface of the base of the
distal phalanx of the thumb.
52.3 Action
52.3.1
Flexes the interphalangeal joint of
the thumb. Continued action, flexes the metacarpophalangeal and carpometacarpal
ar- ticulations.
52.4 Nerve Supply
52.4.1
Anterior interosseous branch of the
median, C8, T1.
52.5 Synergists
52.5.1
Flexor pollicis brevis, adductor
pollicis.
52.6 Category
52.6.1
52.7 View
52.7.1
Anterior View
53 FRONTALIS
(EPICRANIUS)
53.1 Origin
53.1.1
No
bony origin, but arises from the epicranial aponeurosis (galea aponeurilica),
anterior to the coronal suture.
53.2 Insertion
53.2.1
Fib~rs
ale coqtinuous with procerus, corrugiltor supercllil and orblculans oculi below
and the galea aponeuntlca above.
53.3 Action
53.3.1
Elevates
the eyebrows and nasal skin while simultaneously protracting the scalp.
53.4 Nerve Supply
53.4.1
Temporal
branches of the facial nerve (VII).
53.5 Arterial supply
53.5.1
SuRraorbital
and supratrochlear branches of the Qpl,1thalmic artery. The frontal (anterior)
branch of the supertlclal temporal artery.
53.6 Synergists
53.6.1
Occipitalis.
53.7 Antagonists
53.7.1
Procerus,
corrugator supercilii, and orbicularis oculi.
53.8 Category
53.8.1
54 GASTROCNEMIUS
Back Table of Contents References
54.1 Word Derivation
and Pronunciation
54.2 Pronunciation
54.2.1.1GASTROCNEMIUS -
"gas-(")träk-'nE-mE-&s, -tr&k-
54.2.1.2Pronunciation Key
54.2.2
Etymology
54.2.2.1gaster=belly
54.2.2.2kneme=leg
54.2.2.3New Latin, from
Greek gastroknEmE calf of the leg, from gastr- + knEmE shank
54.3 Attachments
54.3.1
Origin
54.3.1.1 Lateral
Head
54.3.1.1.1
Lateral condyle and posterior
surface of femur (knee joint)
54.3.1.1.2
Capsule of knee joint
54.3.1.2 Medial
Head
54.3.1.2.1
Proximal and posterior part of
Medial condyle and adjacent part of femur
54.3.1.2.2
Capsule of knee joint
54.3.2
Insertion
54.3.2.1 Middle
part of posterior surface of calcaneus by means of tendo calcaneus (Achilles
tendon)
54.4 Joints
54.5Ankle (Talocrural)
54.6Knee
(Tibiofemoral)
54.7Tibiofibular
54.8 Action
54.8.1
Plantar flexion (Foot)
54.8.2
Inversion (Foot)
54.8.3
Reversed Origin-Insertion Action
54.8.3.1Flexes
leg at the knee
54.8.3.2Dorsiflexion
of foot increases knee flexion capability.
54.8.4
Note
54.8.4.1Since the
gastrocnemius originates above the knee and the soleus below the knee, the
differentiating factor in testing the two muscles is the knee position during
the test.
54.9 Nerve Supply
54.9.1
Nerve
54.9.1.1Tibial
54.9.2
Roots
54.9.2.1S1
54.9.2.2S2
54.10
Synergists
54.10.1 Soleus
54.10.2 Plantaris
54.10.3 Tibialis
posterior
54.10.4 Peroneus
longus
54.10.5 Peroneus
brevis
54.10.6 Flexor
hallucis longus
54.10.7 Flexor
digitorum longus
54.11
Muscle Tests
54.11.1 GASTROCNEMIUS
54.12
Trigger Points
54.12.1 GASTROCNEMIUS
54.13 Organ Reflexes
54.13.1 Adrenal
54.13.2 Illustrations
54.14
Acupressure/Acupuncture Theory
54.14.1
Organs
54.14.1.1 Pericardium
and Triple Burner
54.14.2 Channels
Discussion
54.14.2.1 Pericardium
(Circulation Sex)
54.14.3 Channel
54.14.3.1 Pericardium
(Circulation Sex) Illustration
54.14.4 Command Points
54.14.4.1 Pericardium
(Circulation Sex)
54.15
Nutritional
54.15.1 Adrenal
concentrate
54.15.2 Nucleoprotein
Extract
54.16
Discussion (Gray)
54.16.1 The Gastrocnemius
is the most superficial muscle, and forms the greater part of the calf. It
arises by two heads, which are connected to the condyles of the femur by
strong, flat tendons. The medial and larger head takes its origin from a
depression at the upper and back part of the medial condyle and from the
adjacent part of the femur. The lateral head arises from an impression on the
side of the lateral condyle and from the posterior surface of the femur
immediately above the lateral part of the condyle. Both heads, also, arise from
the subjacent part of the capsule of the knee. Each tendon spreads out into an
aponeurosis, which covers the posterior surface of that portion of the muscle
to which it belongs. From the anterior surfaces of these tendinous expansions,
muscular fibers are given off; those of the medial head being thicker and
extending lower than those of the lateral. The fibers unite at an angle in the
middle line of the muscle in a tendinous raphé, which expands into a broad
aponeurosis on the anterior surface of the muscle, and into this the remaining
fibers are inserted. The aponeurosis, gradually contracting, unites with the
tendon of the Soleus, and forms with it the tendo calcaneus. 13
54.16.2
54.16.3 Variations.—Absence
of the outer head or of the entire muscle. Extra slips from the popliteal
surface of the femur.
54.16.4 Discussion
54.16.4.1 http://www.bartleby.com/107/129.html
54.16.5 Illustration
54.16.5.1 http://www.bartleby.com/107/illus438.html
54.16.5.2 http://www.bartleby.com/107/illus440.html
54.17
Category
54.17.1 Foot & Toes (Posterior
Superficial Compartment)
54.18
View
54.18.1
Posterior View
55 GEMELLUS INFERIOR (1
of 6 Deep Lateral Rotators of Femur)
55.1 Origin
55.1.1
Superior aspect of the ischial
tuberosity.
55.2 Insertion
55.2.1
With the tendon of obturator intern
us into the medial surface of the greater trochanter of the femur.
55.3 Action
55.3.1
Laterally rotates the extended thigh
at the hip, can also produce horizontal extension. Abducts the flexed thigh.
55.4 Nerve Supply
55.4.1
Sacral plexus, L4, 5, S1.
55.5 Synergists
55.5.1
Piriformis, obturator externus,
obturator internus, quadratus femoris, gemellus superior .
55.6 Category
55.6.1
55.7 View
55.7.1
Posterior View
56 GEMELLUS SUPERIOR (1
of 6 Deep Lateral Rotators of Femur)
56.1 Origin
56.1.1
The outer surface of the ischial
spine.
56.2 Insertion
56.2.1
With the tendon of obturator
internus into the medial surface of the greater trochanter of the femur.
56.3 Action
56.3.1
Laterally rotates the extended thigh
at the hip, can also produce horizontal extension. Abducts the flexed thigh.
56.4 Nerve Supply
56.4.1
Sacral plexus, L5, S1, 2.
56.5 Synergists
56.5.1
Piriformis, obturator externus,
obturator internus, quadratus femoris, gemellus inferior .
56.6 Category
56.6.1
56.7 View
56.7.1
Posterior View
57 GENIOGLOSSUS
57.1 Origin
57.1.1
The
superior mental spines behind the mandibular symphysis, above the origin of
geniohyoid.
57.2 Insertion
57.2.1
Inferior
fibers: By thin aponeurosis, to the upper anterior surface of the hyoid body near
the midline, a few fibers passing between hyoglossus and chondroglossus to
blend with the pharyngeal middle constrictor.
57.2.2
Middle
fibers: The hyodlossal membrane, which is the continuation of the lingual
septum that connects the lingual root to the hyoid bone.
57.2.3
Superior
fibers: The whole length of the ventral surface of the tongue, from root to
apex, intermingling with the intrinsic lingual muscles.
57.3 Action
57.3.1
Forward
traction of the tongue to protrude its apex from the mouth. Acting bilaterally,
depresses the medial part of the tongue, making it concave from side to side.
57.4 Nerve Supply
57.4.1
Hypoglossal
nerve {XII).
57.5 Arterial Supply
57.5.1
Lingual
artery and its branches; dorsal lingual and sublingual rami, tonsillar rami of
the facial artery.
57.6 Synergists
57.6.1
Hyoglossus
and chondroglossus.
57.7 Antagonists
57.7.1
Styloglossus
and palatoglossus.
57.8 Category
57.8.1
58 GENIOHYOID
(SUPRAHYOID)
58.1 Origin
58.1.1
Inferior
mental spine behind mandibular symphysis.
58.2 Insertion
58.2.1
Anterior
aspect of the hyoid bone.
58.3 Action
58.3.1
Elevation
and anterior movement of the hyoid bone. When the hyoid is fixed by contraction
of infrahyoid muscles, it depresses tlie mandible.
58.4 Nerve Supply
58.4.1
Branches
of Cl traveling with the hypoglossal nerve.
58.5 Arterial Supply
58.5.1
Submental
branch of the facial artery, the sublingual branch of the lingual artery.
58.6 Synergists
58.6.1
For
elevation of hyoid: Digastric, mylohyoid and stylohyoid.
58.6.2
For
mandibular depression: Digastric and mylohyoid.
58.7 Antagonists
58.7.1
For
elevation of hyoid: Sternohyoid, omohyoid and thyrohyoid.
58.7.2
For
mandibular depression: Temporalis, masseter and medial pterygoid.
58.7.3
For
hyoid protrusion: Stylohyoid.
58.8 Category
58.8.1
59 GLUTEUS MAXIMUS
59.1 Origin
59.1.1
Posterior gluteal line of ilium,
aponeurosis of erector spinae, dorsal surface of sacrum, coccyx and
sacrotuberous liga- ment.
59.2 Insertion
59.2.1
Gluteal tuberosity of femur and
iliotibial tract of fascia lata.
59.3 Action
59.3.1
Extends thigh at the hip, assists in
laterally rotating the thigh. The upper ':?/3 of the muscle are abductors and
the lower 1/3 is inactive as an abductor or an adductor in the standing
position.
59.3.2
REVERSED ORIGIN-INSERTION ACTION:
When the leg is fixed as in standing, the gluteus maximus is an extensor of the
pelvis on the thigh. In this case, it is a synergist to the abdominal muscles.
59.4 Nerve Supply
59.4.1
Inferior gluteal, L5, 51, 2.
59.5 Synergists
59.5.1
Hamstrings which are placed at a
disadvantage by knee flexion.
59.6 Category
59.6.1
59.7 View
59.7.1
Posterior View
60 GLUTEUS MEDIUS
60.1 Origin
60.1.1
Outer surface of ilium from iliac
crest and posterior gluteal line above to the anterior gluteal line below,
gluteal aponeurosis.
60.2 Insertion
60.2.1
Lateral surface of greater
trochanter.
60.3 Action
60.3.1
Abducts femur at the hip and rotates
it medially. Possible lateral rotation. With gluteus minimus is major lateral
pelvic stabi- lizer. Aids in early activity of hip flexion.
60.4 Nerve Supply
60.4.1
Superior gluteal, L5, 51.
60.5 Synergists
60.5.1
Gluteus minimus, tensor fasciae
latae, upper '2/3 of gluteus maximus.
60.6 Category
60.6.1
60.7 View
60.7.1
Lateral View
61 GLUTEUS MINIMUS
ANT & POST
61.1 Origin
61.1.1
Outer surface of ilium between
anterior and inferior gluteal lines and margin of greater sciatic notch.
61.2 Insertion
61.2.1
Anterior border of greater
trochanter.
61.3 Action
61.3.1
Abducts femur at the hip and rotates
it medially. Lateral pelvic stabilizer. Aids in early activity of hip flexion
61.4 Nerve Supply
61.4.1
Superior gluteal, L5, S1.
61.5 Synergists
61.5.1
Gluteus medius, tensor fasciae
latae, upper ';/3 of gluteus maximus.
61.6 Category
61.6.1
61.7 View
61.7.1
Lateral View
62 GRACILIS
62.1 Origin
62.1.1
Anterior aspect of lower 1/2 of symphysis
pubis and medial margin of inferior ramus of pubis.
62.2 Insertion
62.2.1
Anterior and medial surface of the
shaft of the tibia just below the condyle.
62.3 Action
62.3.1
Adducts and medially rotates thigh.
Flexes and medially rotates leg.
62.3.2
REVERSED
ORIGIN-INSERTION ACTION: When
the thigh is fixed, flexes the pelvis at hip.
62.4 Nerve Supply
62.4.1
Obturator, L2, 3.
62.5 Synergists
62.5.1
Adductor brevis, adductor longus,
adductor mag- nus, pectineus.
62.6 Category
62.6.1
62.7 View
62.7.1
Anterior View
63 HYOGLOSSUS
63.1 Origin
63.1.1
The
whole length of the greater cornu and the front of the body of the hyoid bone.
63.2 Insertion
63.2.1
The
side of the tongue between the styloglossus laterally and the inferior
lingualis muscle medially.
63.3 Action
63.3.1
Depresses
the tongue.
63.4 Nerve Supply
63.4.1
Hypoglossal
nerve (XII).
63.5 Arterial Supply
63.5.1
Lingual
artery and it's dorsal lingual rami.
63.5.2
Tonsillar
rami of the facial-artery.
63.6 Synergists
63.6.1
Chondroglossus.
Also the genioglossus when it contracts bilaterally.
63.7 Antagonists
63.7.1
Styloglossus
and palatoglossus.
63.8 Category
63.8.1
63.9 View
63.9.1
(Note: Styloid process and mastoid portion of
temporal bone are superimposed.)
64 ILIACUS
64.1 Origin
64.1.1
Superior ;?/3 of the iliac fossa,
internal border (inner lip) of iliac crest, anterior sacroiliac, lumbosacral
and iliolumbar liga- ments, ala of sacrum.
64.2 Insertion
64.2.1
Lesser trochanter of femur and for a
short distance below along medial border of shaft.
64.3 Action
64.3.1
Flexes thigh at the hip, minimal
action in lateral rotation of the thigh.
64.3.2
REVERSED ORIGIN-INSERTION ACTION:
When the thigh is fixed, the iliacus muscle flexes the pelvis on the thigh, as
in rising to a sitting position from the supine position (sit up).
64.4 Nerve Supply
64.4.1
Femoral, L2, 3.
64.5 Synergists
64.5.1
Psoas major, adductor longus, adductor
brevis, adductor magnus, rectus femoris.
64.6 Category
64.6.1
64.7 View
64.7.1
Anterior View
65 ILIOCOSTALIS
CERVICIS
65.1 Origin
65.1.1
Superior borders of the angles of the
3rd -6th ribs.
65.2 Insertion
65.2.1
The posterior tubercles of the
transverse processes of the 4th, 5th and 6th cervical vertebrae.
65.3 Action
65.3.1
Acting bilaterally, extension of the
spine. Acting unilaterally, laterally flexes the vertebral column.
65.4 Nerve Supply
65.4.1
Dorsal rami of the spinal nerves,
C6, 7, 8.
65.5 Synergists
65.5.1
Splenius cervicis, semispinalis
cervicis, longis- simus cervicis.
65.6 Category
65.6.1
65.7 View
65.7.1
Posterior View
66 ILIOCOSTALIS
LUMBORUM
66.1 Origin
66.1.1
Anterior surface of a broad and
thick tendon which originates from the sacrum, spinous processes of the lumbar
and 11th and 12th thoracic vertebrae, and from the medial lip of the iliac
crest.
66.2 Insertion
66.2.1
Inferior borders of the angles of
the lower 6 or 7 ribs.
66.3 Action
66.3.1
Acting bilaterally, extension of the
spine, Acting unilaterally, laterally flexes the spine.
66.4 Nerve Supply
66.4.1
Dorsal rami of the spinal nerves.
66.5 Synergists
66.5.1
Longissimus thoracis, quadratus
lumborum.
66.6 Category
66.6.1
66.7 View
66.7.1
Posterior View
67 ILIOCOSTALIS
THORACIS
67.1 Origin
67.1.1
Superior borders of the angles of
lower 6 ribs medial to the tendons of insertion of the iliocostalis lumborum.
67.2 Insertion
67.2.1
Into the angles of the upper 6 or 7
ribs and into the transverse process of the 7th cervical vertebra.
67.3 Action
67.3.1
Acting bilaterally, extension of the
spine. Acting unilaterally, laterally flexes the spine.
67.4 Nerve Supply
67.4.1
Dorsal rami of the spinal nerves.
67.5 Synergists
67.5.1
Iliocostalis lumborum, longissimus
thoracis, spinalis thoracis, semispinalis thoracis.
67.6 Category
67.6.1
67.7 View
67.7.1
Posterior View
68 INCISIVUS LABII
INFERIORIS
68.1 Origin
68.1.1
The
floor of the mandibles incisive fossa, late;ral to the mentalis muscle and
below the emmence of the lateral mclsor tooth.
68.2 Insertion
68.2.1
To
the orbicularis oris; suRerficial fibers reach the !lPex.and body of the
modiolus while deep fibers reach the base and lrlfenor cornu.
68.3 Action
68.3.1
J;\ssis~s
orpicularis o.ris (par~ peripheralis inferior and par margmalis mfenor) m
protrudmg the lips.
68.4 Nerve Supply
68.4.1
Inferior
buccal branches of the facial nerve (VII).
68.5 Arterial Supply
68.5.1
Inferior
labial branch of the facial artery and mental branch from the inferior alveolar
artery.
68.6 Synergists
68.6.1
Orbicularis
oris, pars peripheralis inferior and pars margmalis mfenor
68.7 Antagonist
68.7.1
Buccinator,
.depr~ssor anguli oris, risorius zygomaticus major and zygomaticus mmor.
68.8 Category
68.8.1
68.9 Note
68.9.1
( .denotes modiolus)
69 INCISIVUS LABII
SUPERIORIS
69.1 Origin
69.1.1
Maxilla's
incisive fossa superior to the eminence of the lateral incisor tooth.
69.2 Insertion
69.2.1
To
the orbicularis oris; superficial fibers partly blend with levator ang1l;li
oris and to the intermediate and apical modiolar zones. The deep fibers pass to
the superior cornu and oasis moduli.
69.3 Action
69.3.1
Assists
orbicularis oris (oars peripheralis superior and par marginalis superior)
protrude the lips.
69.4 Nerve Supply
69.4.1
Superior
buccal branches of the facial nerve (VII).
69.5 Arterial Supply
69.5.1
Superior
labial branch of the facial artery.
69.6 Synergists
69.6.1
9rbicularis
oris; pars peripheralis superior and par margmalts superIor.
69.7 Antagonists
69.7.1
Buccinator,
zygomaticus major and minor, risorius, and depressor anguli oris.
69.8 Category
69.8.1
69.9 Note
69.9.1
( .denotes modiolus)
70 INFERIOR
LONGITUDINAL LINGUALIS
70.1 Origin
70.1.1
The
lin~al root with some fibres being connected to the body of the hyOId bone.
70.2 Insertion
70.2.1
Apex
of the tongue.
70.3 Action
70.3.1
Shortens
the and turns the apex and sides downward to make the dorsum convex.
70.4 Nerve Supply
70.4.1
Hypoglossal
nerve (XII).
70.5 Arterial Supply
70.5.1
Lingual
artery and its branches; dorsal lingual and sublingual rami.
70.6 Synergists
70.6.1
For
shortening the tongue: Superior lingualis.
70.7 Antagonist
70.7.1
For
depressing the apex and sides: Superior lingualis.
70.8 Category
70.8.1
71 INFERIOR OBLIQUE
71.1 Origin
71.1.1
The
orbital surface of the maxilla lateral to the nasolacrimal groove.
71.2 Insertion
71.2.1
To
the sclera behind the equator into the posterolateral quadrant of the globe
between the inferior and lateral recti.
71.3 Action
71.3.1
Depresses
the posterior aspect of the eye, hence, rotates the visual axis upwards
(elevation) and laterally (abduction). In the anteroposterior axis it extorts
the eye.
71.4 Nerve Supply
71.4.1
Branch
from the inferior division of the oculomotor nerve (III).
71.5 Arterial Supply
71.5.1
A
branch from the infraorbital artery.
71.6 Synergists
71.6.1
Vertical
axis: Lateral rectus and superior oblique.
71.6.2
Transverse
axis: Superior rectus.
71.6.3
Anteroposterior
axis: Inferior rectus.
71.7 Antagonists
71.7.1
Vertical
axis: Medial rectus, superior rectus, and inferior rectus.
71.7.2
Transverse
axis: Superior oblique and inferior rectus.
71.7.3
Anteroposterior
axis: Superior oblique and superior ltL-t .rectus.
71.8 Category
71.8.1
71.9 Note
71.9.1
(Note: All six extraocular muscles are
involved, and act in concert during an eye movement; synergists and antagonists
depend on the fIXation poin~ of the eye prior to movement.) O J
72 INFERIOR
PHARYNGEAL CONSTRICTOR
72.1 Origin/Insertion
72.1.1
Anterior
attachment:
72.1.1.1 Cricopha:ryngeal part: Side of the
cricoid cartilage
back to the inferior cornu of the thyroid cartilage.
72.1.1.2 Thyropharyngeus part: Oblique line of
the thyroid lamina and a tendinous band behind this to the inferior thyroid
tubercle.. the superior aspect of the cricoid cartilage and tne inferior cornu
of the thyroid cartilage.
72.1.2
Posterior
attachment:
72.1.2.1 Inferior fibres: Blend with the
cricular esophageal fibers.
72.1.2.2 Middle fibres: Posterior median
pharyngeal raphe.
72.1.2.3 Superior fibres: Median pharyngeal
raphe, overlapping the middle pnaryngeal constrictor.
72.2 Action
72.2.1
General
sphincteric and peristaltic action during swalloWIng.
72.3 Nerve Supply
72.3.1
Pharyngeal
branch of the vagus nerve (X), with filaments fromthe cra.nia1 accessory
I;lerve tpat pass through the pharyngeal plexus. CrIcopharyngeus IS also
mnervate;d by recurrent laryngeal and externarbranch of the superIor laryngeal
nerves.
72.4 Arterial Supply
72.4.1
Branches
from the superior thyroid artery and pharyngeal branches from the inferior
thyroid artery.
72.5 Synergists
72.5.1
Superior
and middle pharyngeal constrictors.
72.6 Antagonist
72.6.1
None
72.7 Category
72.7.1
73 INFERIOR RECTUS
73.1 Origin
73.1.1
inferior
margin of optic canal on common annular tendon.
73.2 Insertion
73.2.1
Anteroinferior
margin of the eye into the sclera about 6.5 mm. posterior to the margin of the
cornea.
73.3 Action
73.3.1
Depresses
the anterior of the eye, hence, rotates the eye in the transverse axis
downwards. In the vertical axis it aids in m~d!al rotation (adduction) of the
eye. In the anteroposterior axlS it extorts the eye.
73.4 Nerve Supply
73.4.1
Branch
from the inferior division of the oculomotor nerve (III).
73.5 Arterial Supply
73.5.1
Muscular
rami of the ophthalmic artery and a branch from the infraorbital artery.
73.6 Synergists
73.6.1
Vertical
axis: Medial rectus and superior rectus.
73.6.2
Transverse
axis: Superior oblique.
73.6.3
Anteroposterior
axis: Inferior oblique.
73.7 Antagonists
73.7.1
Vertical
axis: Inferior oblique, lateral rectus and superior oblique.
73.7.2
Transverse
axis: Superior rectus and inferior oblique.
73.7.3
Anteroposterior
axis; Superior rectus and superior oblique.
73.8 Category
73.8.1
73.9 Note
73.9.1
{Note:
All six extraocular muscles are involved, and act in concert duri~g a.n eye
.movement; syn.ergists and anta~onists depend on the flXatlon pomt of the eye
pnor to movement.)
74 INFRASPINATUS
(Rotator Cuff Muscle)
74.1 Origin
74.1.1
Infraspinous fossa of scapula
74.2 Insertion
74.2.1
Posterior aspect of greater tubercle
of humerus, and capsule of shoulder joint.
74.3 Action
74.3.1
Lateral rotation of humerus at the
shoulder. Stabilization of the glenohumeral joint.
74.3.2
REVERSED ORIGIN- INSERTION ACTION:
With the arm fixed, abducts the inferior angle of the scapula.
74.4 Nerve Supply
74.4.1
Suprascapular, C4, 5, 6.
74.5 Synergists
74.5.1
Teres minor, subscapularis,
supraspinatus, del- toid.
74.6 Category
74.6.1
74.7 View
74.7.1
Posterior View
75 INTERNAL ABDOMINAL
OBLIQUE (Anterior Division)
75.1 Origin
75.1.1
Lateral '.?/3 of the
inquinalligament and the anterior 1/3 of the middle (or intermediate) line of
the iliac crest.
75.2 Insertion
75.2.1
Crest of the pubis and the linea
alba by its aponeurosis.
75.3 Action
75.3.1
Acting unilaterally, rotates the
trunk to the same side, and laterally flexes the trunk toward the side of
muscle contraction. Acting bilaterally, flexes the vertebral column,
approximating the anterior thorax and pelvis. Supports and compresses the ab-
dominal viscera. Assists in forced expiration.
75.4 Nerve Supply
75.4.1
Ventral rami of T7 -12, and
iliohypogastric and ilioinquinal nerves, L 1.
75.5 Synergists
75.5.1
Opposite external oblique, rectus
abdominis.
75.6 Category
75.6.1
75.7 View
75.7.1
Lateral View
76 INTERNAL ABDOMINAL
OBLIQUE (Lateral Division)
76.1 Origin
76.1.1
Middle 1/3 of the iliac crest on the
middle line and thoraco lumbar fascia.
76.2 Insertion
76.2.1
Inferior borders of the 1Oth, 11th
and 12th ribs.
76.3 Action
76.3.1
Acting unilaterally, approximates
thorax and pelvis laterally. Contributes to rotation of the trunk on the fixed pelvis
toward the side of contraction.
76.3.2
Acting bilaterally, flexes the trunk
on the pelvis.
76.4 Nerve Supply
76.4.1
Ventral rami of T7 -12, and
iliohypogastric and ilioinquinal nerves, L 1.
76.5 Synergists
76.5.1
: Internal oblique (anterior
division, contralateral ex- ternal oblique, rectus abdominis.
76.6 Category
76.6.1
76.7 View
76.7.1
Lateral View
77 INTERNAL
INTERCOSTALS
77.1 Origin
77.1.1
Superior border of rib below.
77.2 Insertion
77.2.1
Inferior border of rib above.
77.3 Action
77.3.1
Depress the ribs during expiration.
77.4 Nerve Supply
77.4.1
Branches from corresponding
intercostal nerves.
77.5 Synergists
77.5.1
Serratus posterior inferior.
Quadratus lumborum.
77.6 Category
77.6.1
77.7 View
77.7.1
Lateral View
78
INTERSPINALES B90E90
Back
Table of Contents References
78.1 Attachments
78.1.1
Origin and Insertion
78.1.1.1Pairs
of small muscles joining the spinous processes of adjacent vertebrae, one on
each side of the interspinous ligament
78.1.1.2Continuous
in the cervical region extending from the axis to the 2nd thoracic vertebra and
in the lumbar region from the first lumbar vertebra to the sacrum
78.2 Action Illus.
(DSL)
78.2.1
Extension of the spine
78.3 Nerve Supply
78.3.1
Dorsal rami of the spinal nerves
78.4 Synergists
78.4.1
Multifidus
78.4.2
Rotatores,
78.4.3
Intertransversarii
78.5 Muscle Tests
78.5.1
INTERSPINALES
78.6 Trigger Points
78.6.1
INTERSPINALES
78.7 Organ Reflexes
78.7.1
None
78.7.2
Illustrations
78.8 Meridian
78.8.1
None
78.9 Discussion (Gray)
78.9.1
The Interspinales
are short muscular fasciculi, placed in pairs between the spinous processes of
the contiguous vertebra, one on either side of the interspinal ligament. In the
cervical region they are most distinct, and consist of six pairs, the
first being situated between the axis and third vertebra, and the last between
the seventh cervical and the first thoracic. They are small narrow bundles,
attached, above and below, to the apices of the spinous processes. In the thoracic
region, they are found between the first and second vertebra, and sometimes
between the second and third, and between the eleventh and twelfth. In the lumbar
region, there are four pairs in the intervals between the five lumbar vertebras.
There is also occasionally one between the last thoracic and first lumbar, and
one between the fifth lumbar and the sacrum.
78.9.2
Actions- the Interspinales by approximating the spinous
processes help to extend the column.
78.9.3
Illustration-None
78.10
Category
78.10.1
Vertebral Column (Segmental)
78.11
View
78.11.1
Posterior View
78.11.1.1 Illus. (DSL)
79 INTERTRANSVERSARII B91E91
Back
Table of Contents References
79.1 Attachments
79.1.1
Origin and Insertion
79.1.1.1The
intertransversarii consist of pairs of small muscles. These muscles are both
anterior and posterior, on each side of the spine joining the transverse
processes of adjacent vertebrae.
79.1.1.2They
extend from the atlas to the first thoracic vertebra and from the 10th thoracic
vertebra to the last lumbar vertebra.
79.2 Action Illus.
(DSL)
79.2.1
Acting unilaterally, lateral flexion
of the spine
79.3 Nerve Supply
79.3.1
Ventral and dorsal rami of the spinal nerves
79.4 Synergists
79.4.1
Interspinales
79.4.2
Rotatores
79.4.3
Multifidus
79.5 Muscle Tests
79.5.1
INTERTRANSVERSARII
79.6 Trigger Points
79.6.1
INTERTRANSVERSARII
79.7 Organ Reflexes
79.7.1
None
79.7.2
Illustrations
79.8 Meridian
79.8.1
None
79.8.2
Discussion (Gray)
79.8.3
The Intertransversarii
(Intertransversales) are small muscles placed between the transverse
processes of the vertebra. In the cervical region they are best
developed, consisting of rounded muscular and tendinous fasciculi, and are
placed in pairs, passing between the anterior and the posterior tubercles
respectively of the transverse processes of two contiguous vertebra, and
separated from one another by an anterior primary division of the cervical
nerve, which lies in the groove between them. The muscles connecting the
anterior tubercles are termed the Intertransversarii anteriores; those between the posterior tubercles, the Intertransversarii
posteriores, and both sets are
supplied by the anterior divisions of the spinal nerves (Lickley 81). There are seven
pairs of these muscles, the first pair being between the atlas and axis, and
the last pair between the seventh cervical and first thoracic vertebra. In the thoracic
region they are present between the transverse processes of the lower three
thoracic vertebra, and between the transverse processes of the last thoracic
and the first lumbar. In the lumbar region they are arranged in pairs,
on either side of the vertebral column, one set occupying the entire interspace
between the transverse processes of the lumbar vertebræ, the Intertransversarii
laterales; the other set, Intertransversarii
mediales, passing from the
accessory process of one vertebra to the mammillary of the vertebra below. The
Intertransversarii laterales are supplied by the anterior divisions and the
Intertransversarii mediales by the posterior divisions of the spinal nerves
(Lichley, op. cit.).
79.8.4
Actions- the Intertransversarii approximate the transverse
processes, and help to bend the column to one side.
79.9 Category
79.9.1
Vertebral Column (Segmental)
79.10
View
79.10.1
Posterior View
79.10.1.1 Illus. (DSL)
80 INTRINSIC
AURICULAR MUSCLES
80.1 Origin
80.1.1
Helicis
major: Spine of helix.
80.1.2
Helicis
minor: Cavum conchae.
80.1.3
Tragicus:
Superolateral aspect of the tragus.
80.1.4
Antitragicus:
Outer part of the antitragus prominence.
80.1.5
Transverse
auriculae: Eminentia conchae on the cranial aspect of the auricle.
80.1.6
Obliquus
auriculae: Upper and posterior parts of the eminentia conchae on the cranial
aspect of the auricle.
80.2 Insertion
80.2.1
Helicis
major: The anterior border of the helix, where the helixis about to cUlVe back.
80.2.2
Helicis
minor: The crus of commencement of the helix.
80.2.3
Tragicus:
Inferolateral aspect of the tragus.
80.2.4
Antitragicus:
The tail of the helix and the antihelix.
80.2.5
Transverse
auriculae: Eminentia scaphae on the cranial aspect of the auricle.
80.2.6
G
Obliquus auriculae: Eminentia triangularis on the J O .cranial aspect of the
auricle.
80.3 Action
80.3.1
Minimal
action in man.
80.4 Nerve Supply
80.4.1
Lateral
surface muscles; temporal branch of the facial nerve (VII).
80.4.2
Cranial
surface muscles; posterior auricular branch of the facial nerve (VII).
80.5 Arterial Supply
80.5.1
Auric.ular
rami from the.poster.ior auricular branch of the external carotid artery, the
antenor auncular branches of the superficial tempora1 artery, and auricular
branch from the occipital artery.
80.6 Synergists
80.6.1
80.7 Category
80.7.1
81 ISCHIOCAVERNOSUS
81.1 Origin
81.1.1
81.2 Insertion
81.2.1
81.3 Action
81.3.1
81.4 Nerve Supply
81.4.1
81.5 Synergists
81.5.1
81.6 Category
81.6.1
82 LATERAL
CRICOARYTENOID
82.1 Origin
82.1.1
Uppelborder~fthe
cricoid arch.
82.2 Insertion
82.2.1
Ape;x
of the af..Y.tenoid muscular process, just lateral to the posterIor
crIcoarytenoIds attachments.
82.3 Action
82.3.1
Rotates
the arytenoid, thus closing the attached vocal folds (adductor of vocal cords).
82.4 Nerve Supply
82.4.1
Recurrent
laryngeal branch of the vagus nerve (X)
82.5 Arterial Supply
82.5.1
Superior
laryngeal branch of the suRerior thyroid artery and the inferior laryngeal
branch of the inferior thyroId artery
82.6 Synergists
82.6.1
Transverse
arytenoids
82.7 Antagonist
82.7.1
Posterior
cricoarytenoid
82.8 Category
82.8.1
83 LATERAL PTERYGOID
83.1 Origin
83.1.1
Upper
head: Infratemporal crest and lateral surface of tlie greater wing of the
sphenoid
83.1.2
Lower
head: Lateral surface of lateral pterygoid plate
83.2 Insertion
83.2.1
The
depression on the anterior aspect of the m,andibular neck (pteryg9id fo,:e~)
and to the articular capsule and dISC of the temporomanQlbular JOInt
83.3 Action
83.3.1
Aids
in opening the jaw; protrudes the mandible; moves mandible from side to
sIde
83.3.2
Acting
with thy ipsilateral medial pterygoId It rotates the mandIble on a vertIcal
axIS
83.4 Nerve Supply
83.4.1
Branches
from the anterior trunk of the mandibular division of the trigeminal nerve (V3)
83.5 Arterial Supply
83.5.1
Lateral
pterygoid branch of the maxillary artery, a,nd for the upper head, the
accessory meningeal branch of the maxIllary artery
83.6 Synergists
83.6.1
For
opening the jaw: Digastric, mylohyoid and geniohyoid when infrahyoid muscles
contract to fix fiyoid Done, and platysma
83.6.2
For
protrusion: Medial pterygoids. For side-to-side: Masseter
83.7 Antagonists
83.7.1
For
opening the jaw: The anterior fibers of the temporalis, the masseter and medial
pterygoids
83.7.2
For
protrusion: The posterior fibers of the temporalis
83.8 Category
83.8.1
84 LATERAL RECTUS
84.1 Origin
84.1.1
Inferolateral
margin of the optic canal on the common annular tendon with a small tendinous
slip attached to the orbital surface of the greater wing of the sphenoid,
lateral to the annulus
84.2 Insertion
84.2.1
Lateral
margin of the eye into the sclera about 6.9 mm posterior to the margin of the
cornea
84.3 Action
84.3.1
In
the vertical axis it laterally rotates (abducts) the eye
84.4 Nerve Supply
84.4.1
Abducent
nerve (VI)
84.5 Arterial Supply
84.5.1
Muscular
rami from the lacrimal branch of the ophthalmic artery
84.6 Synergists
84.6.1
Superior
and inferior oblique
84.7 Antagonists
84.7.1
Medial
rectus, inferior rectus and superior rectus
84.8 Category
84.8.1
84.9 Note
84.9.1
(No.te: All six extraocular muscles,are
involved, an~ act in concert dun~g a.n. eye,movement; syn,erglsts and
anta~ornsts depend on the flXatlon pomt of the eye pnor to movement.)
85 LATISSIMUS DORSI
85.1 Origin
85.1.1
Broad aponeurosis that originates on
the spinous proces- ses of lower 6 thoracic and all lumbar vertebrae; posterior
crest of ilium, posterior surface of sacrum, lower 3 or 4 ribs, and an
attachment to the inferior angle of the scapula
85.2 Insertion
85.2.1
Flat tendon that twists upon itself
to insert into the intertubercular sulcus of the humerus, just anterior to and
parallel with tendon of pectoralis major
85.3 Action
85.3.1
Extends, retracts and medially
rotates the humerus at the shoulder. Through its action on the humerus it
depresses, retracts and rotates the scapula downwards. Assists in forced
expiration
85.4 Nerve Supply
85.4.1
Thoracodorsal from brachial plexus,
C6, 7, 8
85.5 Synergists
85.5.1
Rhomboids, pectoralis major, teres
major
85.6 Category
85.6.1
85.7 View
85.7.1
Posterior View
86 LEVATOR ANGULI
ORIS(CANINUS)
86.1 Origin
86.1.1
The
canine fossa below the infraorbital foramen
86.2 Insertion
86.2.1
The
modiolus at the angle of the mouth, min.e;lingwith the zygomaticus major, depressor
ang\l;li oris, and of orbicularIs oris. Some superficial fi5ers atfach to the
floor of the lower part of the nasolabiarfurrow
86.3 Action
86.3.1
Raises
the angle of the mouth. Fixes the modiolus
86.4 Nerve Supply
86.4.1
Superior
buccal branches of the facial ne1Ve (VII)
86.5 Arterial Supply
86.5.1
Branches
from facial and infra-orbital arteries
86.6 Synergists
86.6.1
For
elevation of the modiolus: Zygomaticus major
86.6.2
For
elevation of buccal angle: Lateral slip of levator labii superioris alaC?que
nasi, levator labii superioris and zygomatIcus mInor
86.7 Antagonists
86.7.1
Depressor
anguli oris, platysma and orbicularis OrIs
86.8 Category
86.8.1
86.9 Note
86.9.1
( .denotes modiolus)
87 LEVATOR ANI, ILIAC
PART(ILIOCOCCYGEUS)
87.1 Origin
87.1.1
87.2 Insertion
87.2.1
87.3 Action
87.3.1
87.4 Nerve Supply
87.4.1
87.5 Synergists
87.5.1
87.6 Category
87.6.1
88 LEVATOR ANI, PUBIC
PART(PUBOCOCCYGEUS)
88.1 Origin
88.1.1
88.2 Insertion
88.2.1
88.3 Action
88.3.1
88.4 Nerve Supply
88.4.1
88.5 Synergists
88.5.1
88.6 Category
88.6.1
89 LEVATOR LABII
SUPERIORIS
89.1 Origin
89.1.1
The
inferior orbital mar.e;in on both the maxilla and zygomatic bones above the
infraorbital foramen
89.2 Insertion
89.2.1
The
upper lip between the lateral slip of levator labii superioris alaequ.e n.asi
and zygomaticus minor. Also, superficial to the levator anguli OrIS
89.3 Action
89.3.1
Elevates
and everts the upper lip
89.4 Nerve Supply
89.4.1
Superior
buccal branches of the facial nerve (VII)
89.5 Arterial Supply
89.5.1
Branches
from infraorbital artery, branches from the facial and transverse facial
arteries
89.6 Synergists
89.6.1
Lateral
slip of levator labii superioris alaeque nasi, levator anguli oris and
zygomaticus major and minor
89.7 Antagonists
89.7.1
Depressor
anguli oris and orbicularis oris
89.8 Category
89.8.1
90 LEVATOR LABII
SUPERIORIS ALAEQUE NASI
90.1 Origin
90.1.1
Upper
part of the frontal process of the maxillary bone
90.2 Insertion
90.2.1
Medial
slip: The greater alar cartilage and skin of nose
90.2.2
Lateral
slip: Inserts into the lip blending with the orbicularis oris and levator labii
superioris
90.3 Action
90.3.1
Medial
slip: Dilates the nostril; displaces laterally the curvature of the
inferolateral convex circumalar furrow
90.3.2
Lateral
slip: Raises and everts the upper lip. Raises the curvature of the nasolabial
furrows superior part (direct labial tractor)
90.4 Nerve Supply
90.4.1
Superior
buccal branches of the facial nerve (VII)
90.5 Arterial Supply
90.5.1
Lateral
nasal branch from the facial artery, !lIar bra~ches from the superior labial
artery and rami from tlie Infraorbital artery
90.6 Synergists
90.6.1
Medial
slip: Dilator nasi
90.6.2
Latera.1
slip: Levator labii sll;pet:ioris, zygomaticus major and mmor and levator anguh
OrIs
90.7 Antagonsts
90.7.1
Depressor
anguli oris and orbicularis oris
90.8 Category
90.8.1
91 LEVATOR PALPEBRAE
SUPERIORIS
91.1 Origin
91.1.1
91.2 Insertion
91.2.1
91.3 Action
91.3.1
91.4 Nerve Supply
91.4.1
91.5 Synergists
91.5.1
91.6 Category
91.6.1
Eye Ball & Facial Expression
92 LEVATOR SCAPULAE
92.1 Origin
92.1.1
Transverse processes of first four
cervical vertebrae
92.2 Insertion
92.2.1
Vertebral border of scapula between
superior angle and scapular spine
92.3 Action
92.3.1
Elevates the scapula and rotates the
scapula downwards so the glenoid cavity faces inferiorly. Working with the
upper trapezius, elevates and retracts the scapula
92.3.2
REVERSED ORIGIN-INSERTION ACTION:
When scapula is fixed, laterally flexes and slightly rotates cervical spine to
the same side
92.4 Nerve Supply
92.4.1
Dorsal scapular C5, and ventral rami
of C3, 4
92.5 Synergists
92.5.1
Rhomboids and trapezius
92.6 Category
92.6.1
92.7 View
92.7.1
Posterior View
93 LEVATOR VELI
PALATINI
93.1 Origin
93.1.1
The
inferior surface of the apex of the petrous part of the temporal bone, the
uEPer part of the carotid sheath, and the inferior aspect of the cartIlaginous
part of the auditory tube
93.2 Insertion
93.2.1
Blends
in the soft palate and palatine aponeurosis with it's opposite between the two
strands of the palatopharyngeus muscle
93.3 Action
93.3.1
Elevates
the soft palate, closing off the passage between the nasopharynx and oropharynx
93.4 Nerve Supply
93.4.1
Pharyngeal
branch of the vagus (X), with the filaments chiefly from the cranial accessory
nerve that pass through the pharyngeal plexus
93.5 Arterial Supply
93.5.1
Greater
palatine branch of the maxillary artery, the ascending palatine branch of the
facial artery, a variable ramus from tne ascending pharyngeaL artery
93.5.2
93.6 Synergists
93.6.1
None
93.7 Antagonist
93.7.1
None
93.8 Category
93.8.1
93.9 View
93.9.1
(Note:
The maxillary artery is cut.)
94 LEVATORES COSTARUM
BREVES
94.1 Origin
94.1.1
Transverse processes of the 7th
cervical and upper 11 thoracic vertebrae
94.2 Insertion
94.2.1
The outer surface of the rib
immediately below the vertebra from which it takes origin, between the tubercle
and the angle
94.3 Action
94.3.1
Elevate the ribs during inspiration.
Extend the vertebral column, bend it laterally and rotate it slightly toward
the opposite side
94.4 Nerve Supply
94.4.1
From the corresponding thoracic
dorsal rami lateral branches
94.5 Synergists
94.5.1
External intercostals
94.5.2
Serratus posterior superior
94.5.3
Internal intercostals
94.6 Category
94.6.1
94.7 View
94.7.1
Posterior View
95 LEVATORES COSTARUM
LONGI
95.1 Origin
95.1.1
Transverse processes of the 7th -1Oth
thoracic vertebrae
95.2 Insertion
95.2.1
The outer surface of the 2nd rib
below its origin, between the tubercle and the angle
95.3 Action
95.3.1
Elevate the ribs during inspiration.
Extend the vertebral column, bend it laterally and rotate it slightly toward the
opposite side
95.4 Nerve Supply
95.4.1
From the corresponding thoracic
dorsal rami lateral branches
95.5 Synergists
95.5.1
External intercostals, internal
intercostals, levator costarum brevis
95.6 Category
95.6.1
95.7 View
95.7.1
Posterior View
96 LONGISSIMUS
CAPITIS
96.1 Origin
96.1.1
Transverse processes of the 1st -Sth
thoracic vertebrae and the articular processes of the 4th -7th cervical
vertebrae
96.2 Insertion
96.2.1
The posterior margin of the mastoid
process
96.3 Action
96.3.1
Acting bilaterally, extends the
head; acting unilaterally, laterally flexes and rotates the head to the same
side
96.4 Nerve Supply
96.4.1
Dorsal rami of the spinal nerves
96.5 Synergists
96.5.1
Semispinalis capitis, spinalis
capitis, longissimus cervicis
96.6 Category
96.6.1
96.7 View
96.7.1
Posterior View
97 LONGISSIMUS
CERVICIS
97.1 Origin
97.1.1
Transverse processes of the 1 st
-Sth thoracic vertebrae
97.2 Insertion
97.2.1
Transverse processes of the 2nd -6th
cervical ver- tebrae and sometimes to the atlas transverse process
97.3 Action
97.3.1
Acting unilaterally, laterally
flexes the neck
97.3.2
Acting bilaterally, extension of the
neck
97.4 Nerve Supply
97.4.1
Dorsal rami of the spinal nerves
97.5 Synergists
97.5.1
Semispinalis capitis
97.5.2
Semispinalis cervicis
97.5.3
Iliocos- talis cervicis
97.5.4
Longissimus cervicis
97.5.5
Longissimus capitis
97.5.6
Spinalis cervicis
97.5.7
Deep posterior spinal group
97.6 Category
97.6.1
97.7 View
97.7.1
Posterior View
98 LONGISSIMUS
THORACIS
98.1 Origin
98.1.1
The common broad thick tendon with the
iliocostalis lumborum, fibers from the transverse and accessory processes of
the lumbar vertebrae and thoracolumbar fascia
98.2 Insertion
98.2.1
The tips of transverse process of
all thoracic ver- tebrae and the lower 9 or 10 ribs between the tubercles and
angles
98.3 Action
98.3.1
Acting unilaterally, laterally
flexes the vertebral column.
98.3.2
Acting bilaterally, extension of
vertebral column; draws ribs down
98.4 Nerve Supply
98.4.1
Dorsal rami of the spinal nerves
98.5 Synergists
98.5.1
: Iliocostalis lumborum,
iliocostalis thoracis, quad- ratus lumborum
98.6 Category
98.6.1
98.7 View
98.7.1
Posterior View
99 LONGUS CAPITIS
99.1 Origin
99.1.1
Anterior tubercles of transverse
processes of the 3rd -6th cervical vertebrae
99.2 Insertion
99.2.1
Inferior surface of the basilar
portion of the occipital bone
99.3 Action
99.3.1
Acting bilaterally, flexes cervical
vertebrae and head.
99.3.2
Acting unilaterally, rotates and
laterally flexes cervical vertebrae and head to the same side
99.4 Nerve Supply
99.4.1
Ventral rami of C1, 2, 3
99.5 Synergists
99.5.1
: Longus colli, sternocleidomastoid,
scalenus group, suprahyoid, infrahyoid and the platysma
99.6 Category
99.6.1
99.7 View
99.7.1
Anterior View
100
LONGUS CAPITIS ANTERIOR
100.1
Origin
100.1.1
100.2
Insertion
100.2.1
100.3
Action
100.3.1
100.4
Nerve Supply
100.4.1
100.5
Synergists
100.5.1
100.6
Category
100.6.1
101
LONGUS COLLI
101.1
Origin
101.1.1 INFERIOR
OBLIQUE PART: Ist, 2nd or 3rd thoracic vertebral bodies
101.1.2 SUPERIOR
OBLIQUE PART: Anterior tubercles of 3rd, 4th and Sth cervical transverse
processes
101.1.3 VERTICAL
PART: Anterior aspects of the Sth, 6th and 7th cervical and 1st, 2nd and 3rd
thoracic vertebral bodies
101.2
Insertion
101.2.1 INFERIOR
OBLIQUE PART: Anterior tubercles of the Sth, 6th or 7th cervical transverse
processes
101.2.2 SUPERIOR
OBLIQUE PART: Anterolateral surface of the atlanta anterior tubercle, anterior
tubercle
101.2.3 VERTICAL
PART: Anterior aspects of the 2nd, 3rd and 4th cervi- cal vertebral bodies
101.3
Action
101.3.1 Acting
bilaterally, flexes cervical vertebrae. Acting unilaterally, assists in
rotation to opposite side and lateral flexion
101.4
Nerve Supply
101.4.1 Ventral
rami of C2 -6
101.5
Synergists
101.5.1 Scalenus
group, sternocleidomastoid, longus capitis, suprahyoid, infrahyoid and the
platysma
101.6
Category
101.6.1
101.7
View
101.7.1
Anterior View
102
LUMBRICALS (FOOT)
Back Table of Contents References
102.1
Attachments
102.1.1 Attachments
102.1.1.1 Origin
102.1.1.1.1
The four Lumbricals attach to the
medial aspect of the four tendinous slips (which attach to the 2nd
thru 5th digits) of the flexor digitorum longus tendon near where
they branch from the main tendon
102.1.1.2 Insertion
102.1.1.2.1
On the medial side of the proximal
phalanx, into the dorsal expansions of the tendons to the extensor digitorum
longus of the 2nd .5th toes
102.2
Action
102.2.1 Extends
interphalangeal joints
102.2.2 Assists
in flexing metatarsophalangeal joints of the 2nd -5th toes
102.3
Nerve Supply
102.3.1 1st
Lumbrical
102.3.1.1 Nerve
102.3.1.1.1 Medial
plantar
102.3.1.2 Roots
102.3.1.2.1
L4
102.3.1.2.2
L5
102.3.1.2.3
S1
102.3.1.2.4
S2
102.3.1.2.5
S3
102.3.2 2nd,
3rd, 4th Lumbricals
102.3.2.1 Nerve
102.3.2.1.1 Lateral
plantar
102.3.2.2 Roots
102.3.2.2.1 S2
102.3.2.2.2
S3
102.4
Synergists
102.4.1 Flexor
digitorum brevis (metatarsophalangeal articulation)
102.4.2 Flexor
digitorum longus (metatarsophalangeal articulation)
102.4.3 Extensor
digitorum longus (extensor function)
102.4.4 Extensor
digitorum brevis (extensor function)
102.4.5 Dorsal
Interossei
102.4.6 Plantar
Interossei
102.5
Muscle Tests
102.5.1
102.6
Trigger Points
102.6.1
102.7
Discussion (Gray)
102.7.1 The Lumbricales
are four small muscles, accessory to the tendons of the Flexor digitorum longus
and numbered from the medial side of the foot; they arise from these tendons,
as far back as their angles of division, each springing from two tendons,
except the first. The muscles end in tendons, which pass forward on the medial
sides of the four lesser toes, and are inserted into the expansions of the
tendons of the Extensor digitorum longus on the dorsal surfaces of the first
phalanges. 21
102.7.2 Variations.—Absence
of one or more; doubling of the third or fourth. Insertion partly or wholly
into the first phalanges.
102.7.3 Discussion
102.7.3.1 http://www.bartleby.com/107/131.html
102.7.4 Illustration
102.7.4.1 http://www.bartleby.com/107/illus444.html
102.8
Category
102.8.1 Intrinsic Foot (Plantar 2nd
Layer)
102.9
View
102.9.1
Plantar View (2nd Plantar
Layer)
103
LUMBRICALS (HAND)
103.1
Origin
103.1.1 Tendons
of flexor digitorum profundus in center of palm
103.2
Insertion
103.2.1 Around
the radial side of the metacarpal bone and into the extensor expansion
103.3
Action
103.3.1 Principal
extensors of the interphalangeal joints. Weak flexor of the metacarpophalangeal
joints
103.4
Nerve Supply
103.4.1 1
st and 2nd lumbricals from 3rd and 4th palmar digital branches of the median
nerve. 3rd and 4th lumbricals from deep branch of the ulnar nerve, C8, T1
103.5
Synergists
103.5.1 Dorsal
interossei, palmar interossei, flexor digitorum profundus, flexor digitorum
superficialis
103.6
Category
103.6.1
103.7
View
103.7.1
Anterior View
104
MASSETER
104.1
Origin
104.1.1 Superficial layer: Zygomatic process of
the maxillary bone and the anterior 2/3 of tlle inferior border of the
zygomatic arch
104.1.2 Dee-p layer: Posterior li3 of inferior
border and medial surface of zygomatic arch
104.2
Insertion
104.2.1 Superficial layer: Angle of mandible
(continuous with medial pte.rygoid) ana lower posterior 1/2 of the lateral
surface of ItS ramus
104.2.2 Deep layer: Upper part of the
mandibular ramus and lateral surface of coronoid process
104.3
Action
104.3.1 Closes jaw, forms mandibular sling with
the medial pterygoid.
104.3.2 Minimal action in side-to-side,
protraction and retraction movements
104.4
Nerve Supply
104.4.1 Masseteric branch from the anterior
trunk of the mandibular division of the trigeminal nerve (V3)
104.5
Arterial
Supply
104.5.1 Masseteric branch of maxillary artery
and branches froth the facial and transverse facial arteries
104.6
Synergists
104.6.1 The masseter and medial pterygoid act
together forming the mandibular sling. Temporalis muscle
104.7
Antagonists
104.7.1 Digastric, mylohyoid and geniohyoid
when InfrahyoId muscles contract to flX hyoId bone
104.8
Category
104.8.1
105
MEDIAL PTERYGOID
105.1
Origin
105.1.1 Deep attachments
105.1.1.1 Medial aspect of the lateral pterygoid
plate an<;l gI:ooved surface of the pyra~idal process of the palatine bone
105.1.2 Superficial attachment
105.1.2.1 Lateral surfaces of the pyra.midal
proce.ss of the palatine bone and the maxIllary tuDeroslty
105.2
Insertion
105.2.1 A strong tendinous lamina
inferoposterior to the medial surfaces of the mandibular ramus and angle
105.3
Action
105.3.1 Closes the jaw. Forms mandibular slinK
with masseter muscle. Acting with tile ipsilateral lateral pterygoid, it
rotates the mandible to the opposite slGe
105.4
Nerve Supply
105.4.1 Branches from the anterior trunk of the
mandibular division of the trigeminal nerve (V3)
105.5
Arterial
Supply
105.5.1 Branches from maxillary artery; Medial
pterygoid artery and accessory meningeal artery
105.6
Synergists
105.6.1 For closing the jaw; Masseter and
anterior fibers of temporahs
105.7
Antagonists
105.7.1 For closing the jaw; Mylohyoid,
digastric and geniohyoid when infrahyoid muscles contract to fix hyoidDone
105.8
Category
105.8.1
105.9
View
105.9.1
(Note: Zygomatic bone and ramus of mandible
have been removed).
106
MEDIAL RECTUS
106.1
Origin
106.1.1 Superomedial, medial and inferomedial
margins of the optic canal on the common annular tendon
106.2
Insertion
106.2.1 Anteromedial margin of the eye into the
sclera about 5.5 mm posterior to the margIn of the cornea
106.3
Action
106.3.1 In the vertical axis it medially
rotates (adducts) the eye
106.4
Nerve Supply
106.4.1 Branch from the inferior division of
the oculomotor nerve (III)
106.5
Arterial
Supply
106.5.1 Muscular rami from the ophthalmic
branch of the internal carotid artery
106.6
Synergists
106.6.1 Superior and inferior rectus
106.7
Antagonists
106.7.1 Lateral rectus, superior and inferior
oblique
106.8
Category
106.8.1
106.9
106.9.1
(Note: All six extraocular muscles are
involved, and act in concert during an eye movement; synergists and antagonists
depend on the fIXation point of the eye prior to movement.)
107
MENTALIS
107.1
Origin
107.1.1 From the incisive fossa of the mandible
107.2
Insertion
107.2.1 The skin of the chin
107.3
Action
107.3.1 Raises the mental tissues, mentolabial sulcus
and base of the lower lip
107.4
Nerve Supply
107.4.1 Mandibular marginal branch of the
facial nerve (VII)
107.5
Arterial
Supply
107.5.1 Mental branch of inferior alveolar
artery and inferior labial and submental branches of the facial artery
107.6
Synergists
107.6.1 Levator anguli oris and zygomaticus
major
107.7
Antagonists
107.7.1 Depressor labii inferioris and
depressor anguli OrIs
107.8
Category
107.8.1
108
MIDDLE PHARYNGEAL CONSTRICTOR
108.1
Origin/Insertion
108.1.1 Anterior attachments
108.1.1.1 Chondropharyngeal part: The lesser
hyoid
c.ornu ana the lower part of the stylohyoid ltgament
108.1.1.2 Ceratopha!'Jngeal part: The whole upI?er
border of tlie greafer cornu of the hyoid bone
108.1.2 Posterior attachment
108.1.2.1 The posterior median pharypgeal raphe.
108.1.2.2 Superior:ly, fib.ers oyerlaRPing the
superIor pharyngeal constrIctor; ferlorly, libers blend with the inferior
pharyngeal constrictor
108.2
Action
108.2.1 General sphincteric and peristaltic
action during swalloWIng
108.3
Nerve Supply
108.3.1 Pharyn~eal branch of the vagus nerve
(X), with filaments from the crania1 accessory nerve thaI pass throug1i the
pharyngeal plexus
108.4
Arterial
Supply
108.4.1 Ascending pharyngeal artery, ascending
Ralatine and tonsillar branches of the facial artery; the dorsal lingual branch
of the lingual artery
108.5
Synergists
108.5.1 Inferior and superior pharyngeal
constrictors
108.6
Antagonist
108.6.1 Stylopharyngeus dilates the pharynx
108.7
Category
108.7.1
109
MULTIFIDUS
109.1
Origin
109.1.1 A
series of pairs of small muscles extending the full length of the spine just
superlicial to the rotatores and each spanning 2 or 3 intervertebral spaces
before inserting
109.1.2 Posterior
surface of the sacrum, the dorsal end of the iliac crest, the mamillary and
transverse processes of the lumbar and the thoracic vertebrae and the articular
processes of the 4th -7th cervical vertebrae
109.2
Insertion
109.2.1 Spinous
processes of all the vertebrae except the atlas
109.3
Action
109.3.1 Acting
unilaterally, lateral flexion and rotation to the opposite side. Acting
bilaterally, extension of the spine
109.4
Nerve Supply
109.4.1 Dorsal
rami of the spinal nerves
109.5
Synergists
109.5.1 Rotatores,
interspinales, intertransversarii groups
109.6
Category
109.6.1
109.7
View
109.7.1
Posterior View
110
MUSCULUS UVULAE
110.1
Origin
110.1.1 Posterior nasal spine of the palatine bone
and to the palatine aponeurosis
110.2
Insertion
110.2.1 Uvular mucosa
110.3
Action
110.3.1 Elevation and retraction of the uvula
110.4
Nerve Supply
110.4.1 Pharyngeal branch of the vagus (X),
with the filaments chiefly from the cranial accessory nerve that pass through
the pharyngeal plexus
110.5
Arterial
Supply
110.5.1 Greater palatine branch of the
maxillary artery, the ascending palatine branch of the facial artery, a
variable ramus from the ascending pharyngeal artery
110.6
Synergists
110.6.1 None
110.7
Antagonist
110.7.1
110.8
Category
110.8.1
110.9
View
110.9.1
(Note: Maxillary artery is cut.)
111
MYLOHYOID (SUPRAHYOID)
111.1
Origin
111.1.1 The mylohyoid line on the mandible
111.2
Insertion
111.2.1 Posterior fibers
111.2.1.1 Anterior aspect of the hyoid body near
its lower border
111.2.2 Middle and anterior fibers
111.2.2.1 Decussate in a median fibrous raphe
stretching from the mandibular symphysis to the hyold,bone
111.3
Action
111.3.1 Elevation of the floor of mouth as
during mastication and swallowing
111.3.2 Elevates the hyoid bone or depresses
the mandible
111.4
Nerve Supply
111.4.1 Mylohyoid branch of the inferior
alveolar nerve from the trigeminal nerve (V3)
111.5
Arterial
Supply
111.5.1 Mylohyoid branch of the inferior
alveolar artery, the submental branch of the facial artery and the sublingual
brancn of the lingual artery
111.6
Synergists
111.6.1 Digastric, stylohyoid and geniohyoid
111.7
Antagonists
111.7.1 Infrahyoid muscles (sternohyoid,
omohyoid, and ~ thyrohyoId)
111.8
Category
111.8.1
111.9
VIew
111.9.1
(Note: The mandible and zygomatic arch have
two different sagittal sectIons).
112
NASALIS, ALAR PORTION
112.1
Origin
112.1.1
112.2
Insertion
112.2.1
112.3
Action
112.3.1
112.4
Nerve Supply
112.4.1
112.5
Synergists
112.5.1
112.6
Category
112.6.1
113
NASALIS (COMPRESSOR & DILATOR NARIS)
113.1
Origin
113.1.1 Compressor naris
113.1.1.1 The maxilla, lateral to its incisive
fossa
113.1.2 Dilator naris
113.1.2.1 The maxilla, inferomedial to and
partially blended with the compressor
113.2
Insertion
113.2.1 Compressor naris
113.2.1.1 The expanded aponeurosis, contInuous
with that on the opposite side, and also blends with the aponeurosis of
procerus
113.2.2 Dilator naris
113.2.2.1 The cartilaginous ala nasi
113.3
Action
113.3.1 Compressor naris
113.3.1.1 Compresses the nasal aperture at the
junction of the vestibule and nasal cavity
113.3.2 Dilator naris
113.3.2.1 Depresses the ala laterally, widening the
anterIor nasal aperture
113.4
Nerve Supply
113.4.1 Superior buccal branches of the facial
nerve(VII)
113.5
Arterial
Supply
113.5.1 Lateral nasal branch of the facial and
alar ram~ from t~e superior labial branch of the facial artery. Rami from the
Infraorbital artery
113.6
Synergists
113.6.1 For dilation of nasal cavity; the
medial slips of the labii superioris alaeque nasi, and depressor septi
113.7
Antagonist
113.7.1 None
113.8
Category
113.8.1
114
OBLIQUE ARYTENOID & ARYEPIGLOTTICUS
114.1
Origin/Insertion
114.1.1 Run obliquely from the muscular process
of one ary.tenoid to the other (oblique arytenoid) and from the apex into the
aryepiglottic fold (aryepiglottlcus)
114.2
Action
114.2.1 Oblique arytenoids
114.2.1.1 Adduction of the aryepiglottic fold and
vocal cords, acting as a sphincter of the laryngeal inlet
114.2.2 Ary~piglotticus
114.2.2.1 Appt:oximates the arytenoid cartIIages
to the epIglottIc tubercle
114.3
Nerve Supply
114.3.1 Recurrent laryngeal branch of the vagus nerve (X)
114.4
Arterial
Supply
114.4.1 Superior laryngeal branch 9f th.e
superi9r thyroId artery and mfenor laryngeal branch of the mfenor tfiyrold
artery
114.5
Synergists
114.5.1 Transverse arytenoids
114.6
Antagonist
114.6.1 Thyroepiglottic
114.7
Category
114.7.1
115
OBLIQUUS CAPITIS INFERIOR
115.1
Origin
115.1.1 The
apex of the spinous process of the axis
115.2
Insertion
115.2.1 The
inferior and dorsal part of the transverse process of the atlas
115.3
Action
115.3.1 Rotates
the atlas, turning the face toward the same side
115.4
Nerve Supply
115.4.1 Suboccipital
nerve dorsal ramus C1
115.5
Synergists
115.5.1 Longissimus
capitis, rectus capitis posterior major
115.6
Category
115.6.1
115.7
View
115.7.1
Posterior View
116
OBLIQUUS CAPITIS SUPERIOR
116.1
Origin
116.1.1 The
superior surface of the transverse process of the atlas
116.2
Insertion
116.2.1 Between
the superior and inferior nuchal lines of the occipital bone, lateral to the
semispinalis capitis
116.3
Action
116.3.1 Extension
and lateral flexion of the head at the neck
116.4
Nerve Supply
116.4.1 Suboccipital
nerve, dorsal ramus C1
116.5
Synergists
116.5.1 Rectus
capitis posterior minor, rectus capitis posterior major, longissimus capitis,
semispinalis capitis
116.6
Category
116.6.1
116.7
View
116.7.1
Posterior View
117
OBTURATOR EXTERNUS (1
of 6 Deep Lateral Rotators of Femur)
117.1
Origin
117.1.1 Outer
surface of obturator membrane and the margin of bone immediately around the
medial side of the obturatorforamen, from the rami of the pubis and the
inferior ramus of the ischium
117.2
Insertion
117.2.1 Trochanteric
fossa on the medial aspect of the greater trochanter
117.3
Action
117.3.1 Lateral
rotation of femur at the hip
117.4
Nerve Supply
117.4.1 Obturator,
L3,4
117.5
Synergists
117.5.1 Piriformis
117.5.2 Superior
and inferior gemelli
117.5.3 Obturator
internus
117.5.4 Quadratus
femoris
117.6
Category
117.6.1
117.7
View
117.7.1
Posterior View
118
OBTURATOR INTERNUS (1
of 6 Deep Lateral Rotators of Femur)
118.1
Origin
118.1.1 Pelvic
surface of obturator membrane and bony margin of the obturator foramen
118.2
Insertion
118.2.1 Medial
surface of the greater trochanter of the femur
118.3
Action
118.3.1 Laterally
rotates the extended thigh at the hip can also produce horizontal extension
118.3.2 Abducts
the flexed thigh
118.4
Nerve Supply
118.4.1 Sacral
plexus, L5, S1, 2
118.5
Synergists
118.5.1 Piriformis,
obturator externus, quadratus femoris, superior and inferior gemelli
118.6
Category
118.6.1
118.7
View
118.7.1
Posterior View
119
OCCIPITALIS (EPICRANIUS)
119.1
Origin
119.1.1 Lateral two thirds of the highest
nuchal line of occipital bone and mastoid part of temporal bone
119.2
Insertion
119.2.1 The cranial aponeurosis, galea
aponeuritica
119.3
Action
119.3.1 Retract sca1[); through the galea
aponeuritica, it assists in raising the upper eyeltos
119.4
Nerve Supply
119.4.1 Occip-ital branch of the posterior auricular
nerve from the facial nerve (VII)
119.5
Arterial
Supply
119.5.1 Posterior auricular artery and
occipital artery
119.6
Synergists
119.6.1 Frontalis
119.7
Antagonist
119.7.1 Platysma (indirectly)
119.8
Category
119.8.1
120
OMOHYOID SUPERIOR & INFERIOR (INFRAHYOID)
120.1
Origin
120.1.1 Inferior belly
120.1.1.1 Upper scapular border, near the suprascapular
notch and occasIonally tlie superior transverse scapular ligament
120.1.2 Superior belly
120.1.2.1 Intermediate tendon, located near the
lateral border of the sternohyoid. The intermediate tendon is attached to the
clavicle and first rib by a sling of deep cervical fascia
120.2
Insertion
120.2.1 Inferior belly
120.2.1.1 Intermediate tendon, located near the
lateral border of the sternohyoId
120.2.2 Su~erior belly
120.2.2.1 The lower border of the hyoid body,
just lateral to the sternohyoid attachment
120.3
Action
120.3.1 Both bellies lowers the hyoid after it
has been raised
120.4
Nerve Supply
120.4.1 Inferior belly
120.4.1.1 Inferior ramus of the ansa cervicalis
(C2, C3)
120.4.2 Superior belly
120.4.2.1 Superior ramus of ansa cervicalis (Cl,
C2)
120.5
Arterial
Supply
120.5.1 Inferior belly
120.5.1.1 Suprascapular artery
120.5.2 Superior belly
120.5.2.1 Superior and inferior thyroid arteries
120.6
Synergists
120.6.1 Sternohyoid, sternothyroid and
thyrohyoid
120.7
Antagonists
120.7.1 Suprahyoid muscles (e.g., digastric)
120.8
Category
120.8.1
121
OPPONENS DIGITI MINIMI
121.1
Origin
121.1.1 Hamulus
or hook of the hamate bone and flexor retinaculum
121.2
Insertion
121.2.1 Entire
length of ulnar border of 5th metacarpal
121.3
Action
121.3.1 Flexes
and slightly laterally rotates the 5th metacarpal. Helps to cup the palm of the
hand
121.4
Nerve Supply
121.4.1 Deep
branch of ulnar nerve, C8, T1
121.5
Synergists
121.5.1 Flexor
digiti minimi brevis, abductor digiti minimi
121.6
Category
121.6.1
121.7
View
121.7.1
Anterior View -
122
OPPONENS POLLICIS
122.1
Origin
122.1.1 Flexor
retinaculum and tubercle of trapezium bone
122.2
Insertion
122.2.1 Radial
side of entire length of first metacarpal bone
122.3
Action
122.3.1 Flexes
and abducts the first metacarpal with slight medial rotation
122.4
Nerve Supply
122.4.1 Median,
C8, T1 and commonly a ramus from the deep terminal branch of ulnar
122.5
Synergists
122.5.1 Abductor
pollicis, adductor pollicis
122.6
Category
122.6.1
122.7
View
122.7.1
Anterior View
123
ORBICULARIS OCULI
123.1
Origin
123.1.1 Orbital part
123.1.1.1 Nasal part of the frontal bone lthe frontal p;rocess of the maxilla
and the media palpebral ligament
between them
123.1.2 Palpebral part
123.1.2.1 Medial palpebral ligament
123.1.3 Lacrimal part
123.1.3.1 Just Rosterior of the lacrimal sac to
the upper part of the lacrimal crest
123.2
Insertion
123.2.1 Orbit.al part
123.2.1.1 Surround~ orbi~ and &preads into
the anterIOr
temporal regIon, Infraorbital cheek and superciliary region. (Nofe: no bony
attachments)
123.2.2 Palpebral part
123.2.2.1 Across eyelids anterior to the orbital
septum, inserting into the lateral palpebral raphe
123.2.3 Lacrimal part
123.2.3.1 S~perior and inferior tarsi and the
lateral palpebral rapfie
123.3
Action
123.3.1 Orbital part
123.3.1.1 Protrusion of the eyebrows, and closes
the eyelids, usually a voluntary action
123.3.2 Palpebral part
123.3.2.1 Closes lids during blinking
123.3.3 Lacrimal part
123.3.3.1 Draws lids and lacrimal papillae medially,
also compresses the lacrimal sac
123.4
Nerve Supply
123.4.1 Temporal & zygomatic branches
facial nerve (VU)
123.5
Arterial
Supply
123.5.1 Zygomatico-orbital artery, palpebral
branches from the ophthalmic and lacrimal arteries
123.6
Synergists
123.6.1 For protrusion; corrugator supercilii
and procerus
123.7
Antagonists
123.7.1 Levator palRebrae superioris for
closing the eyelids and the frontalis muscle lor protrusIon of the eyebrows
123.8
Category
123.8.1
124
ORBICULARIS ORIS
124.1
Origin/Insertion
124.1.1 l:atera~
attac~l.tlel!ts
124.1.1.1 La.bial
aspect of the modiol\!s with fibers Interdlgltat~ng ~lth those from thy
buc.clnatorl depresso.r an~11 OrIS, levator angulI OrIS ana zygomaticus major
124.1.2 Pars
peripheralis superior
124.1.2.1 The
highest fibers extend to th.e nasorabial s~lc~s, nasal .!lla anq s.eptum .and
are reinforced from InCISlVUS labll superlorls and Its fibers from the
contralateral side
124.1.3 Pars
peripheralis inferior
124.1.3.1 The
lowest fibers to the mento1abial sulcus. Reinforcement from incisivus labii
inferior and fibers from the contralateral side
124.1.4 Pars
marginalis inferior and superior
124.1.4.1 Fibers
meet and interlace with their contralateral partners in the red- lipped dermis
124.2
Action
124.2.1 Direct
closure of lips by its deep fibers. b!ipg lips tog.ether and als~ Qrotrudes
then forward Dy superficial, prIncipally decussatlng fibers
124.3
Nerve Supply
124.3.1 Buccal
branches of the facial nerve (VII)
124.4
Arterial Supply
124.4.1 Superior
and inferior labial branch of the facial artery and mental branches of the
inferior alveolar artery
124.5
Synergists
124.5.1 lncisivus
labii superior, incisivus labii inferior and mentalis
124.6
Antagonists
124.6.1 La;te~al
slip of leyator lajJii suRerioris alaequ.e na~i, levator lab 11 su.perlorls,
zygomaticus mInor, levator angulI OrIS, zygomati~s major, depressor labii
inferioris, depressor anguli oris, ana buccInator
124.7
Category
124.7.1
124.8
Note
124.8.1
(Denotes modiolus)
125
PALATOGLOSSUS (Palatoglossal arch; Anterior pillar)
125.1
Origin
125.1.1 The oral surface of the palatine
aponeurosis, where it is continuous with its muscle fibers from the
contralateral side
125.2
Insertion
125.2.1 Anterior to the tonsil to the side of
the tongue, with fibres over the lingual dorsum, and others deep to intermingle
with the transverse 1ingualis
125.3
Action
125.3.1 Elevates the root of the tongue and
approximates the palatoglossal arch, closing the ismus of the fauces, thus
shutting off the oral cavity from oropharynx
125.4
Nerve Supply
125.4.1 Pharyngeal branch of the vagus nerve
(X), with filaments chiefly from the cranial accessory nerve that pass through
the pharyngeal plexus
125.5
Arterial
Supply
125.5.1 Greater palatine branch of the
maxillary artery, the ascending palatine and tonsillar branches of the facial
artery, the dorsal lingual branches of the lingual artery
125.6
Synergists
125.6.1 For elevation of the tongue
125.6.1.1 Styloglossus
125.7
Antagonists
125.7.1 For elevation of tongue base
125.7.1.1 Supra-and infra-hyoid muscles
125.8
Category
125.8.1 Tongue & soft
palate
126
PALATOPHARYNGEUS (Palatopharyngeal
arch; Posterior pillar)
126.1
Origin
126.1.1 Anterior
fibres
126.1.1.1 The
posterior border of the hard palate and from the palatine aponeurosis with the fibres
interdigitating with it's opposite across the midline, between the levator veli
pa1atine
126.1.2 Posterior
fibres
126.1.2.1 Posterior
to the levator veli palatini, the pharyngeal aspect of the palate and joining
the posterior band of the opposite muscle in the midline
126.1.3 United
fibres
126.1.3.1 At
the soft palates posterolateral border the anterior and posterior fibres unite
with the salpingopharyngeus muscle
126.2
Insertion
126.2.1 Poster~or
border .of the t~yroid cart.ila,ge, pharyngeal fibrous tissue and fibres
crossmg the midlme postenorly, decussating with it's opposite muscle
126.3
Action
126.3.1 Elevates
and draws pharnyx forward and medially during swallowing
126.4
Nerve Supply
126.4.1 Pharyngeal
branch of the vagus nerve (X), with filaments chiefly from the cranial
accessory nerve that pass through the paryngeal plexus
126.5
Arterial Supply
126.5.1 Ascending
pha~geal artery, asce~ding palatine and tonsillar branches of facial and
maxillary arteries, greater palatine, pharyngeal, and the artery of the
pterygoid canal
126.6
Synergists
126.6.1 Salpingopharyngeus
and stylopharyngeus act as pharyngeal elevators
126.7
Antagonists
126.7.1 Infrahyoid
muscles lower pharynx during late stages of swallowing
126.8
Category
126.8.1 Pharynx
longitudinal layer & soft palate
126.9
View
126.9.1
(Note: Salpingopharyngeus muscle is
also illustrated).
127
PALMAR INTEROSSEI (HAND)
127.1
Origin
127.1.1 Sides
of the metacarpals l' 2, 4 and 5
127.2
Insertion
127.2.1 Extensor
expansion of the respective digit with pos- sible attachment to the base of the
proximal phalanx
127.3
Action
127.3.1 Adducts
the thumb, index, ring and little fingers toward the middle finger. All four
assist in flexing the proximal phalanges of the thumb, index, ring and little
fingers at the metacarpophalan- geal joints, and in extending the middle and
distal phalanges
127.4
Nerve Supply
127.4.1 Deep
branch of the ulnar nerve, C8, T1
127.5
Synergists
127.5.1 Dorsal
interossei, lumbricals, extensor indicis, flexor digitorum superficialis,
flexor digitorum profundus
127.6
Category
127.6.1
127.7
View
127.7.1
Anterior View
128
PALMARIS BREVIS
128.1
Origin
128.1.1
128.2
Insertion
128.2.1
128.3
Action
128.3.1
128.4
Nerve Supply
128.4.1
128.5
Synergists
128.5.1
128.6
Category
128.6.1
129
PALMARIS LONGUS
129.1
Origin
129.1.1 Common
flexor tendon from medial epicondyle of humerus
129.2
Insertion
129.2.1 Flexor
retinaculum and palmar aponeurosis
129.3
Action
129.3.1 Flexes
hand at the wrist
129.4
Nerve Supply
129.4.1 Median
C7, 8
129.5
Synergists
129.5.1 Flexor
carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis
129.6
Category
129.6.1
129.7
View
129.7.1
Anterior View
130
PECTINEUS
130.1
Origin
130.1.1 Superior
surface of the pubis, the pectineal line between iliopectineal eminence and
pubic tubercle
130.2
Insertion
130.2.1 Pectineal
line of femur, from lesser trochanter to linea aspera
130.3
Action
130.3.1 Adduction
of thigh at hip
130.3.2 Assistance
in thigh flexion and medial rotation at the hip
130.4
Nerve Supply
130.4.1 Femoral
and obturator nerves, L2, 3, 4
130.5
Synergists
130.5.1 Adductor
brevis, adductor longus, adductor mag- nus, gracilis
130.6
Category
130.6.1
130.7
View
130.7.1
Anterior View
131
PECTORALIS MAJOR CLAVICULAR
131.1
Origin
131.1.1 Anterior
surface of the medial 1/2 of the clavicle
131.2
Insertion
131.2.1 Lateral
lip of the intertubercular sulcus of the humerus
131.2.2 Crest
of greater tubercle
131.3
Action
131.3.1 Flexion,
adduction, horizontal flexion and medial rotation of the humerus at the
shoulder
131.4
Nerve Supply
131.4.1 Lateral
pectoral, C5, 6
131.5
Synergists
131.5.1 Biceps
brachi, pectoralis major (sternal division), latissimus dorsi, deltoid
(anterior division)
131.6
Category
131.6.1
131.7
View
131.7.1
Anterior View
132
PECTORALIS MAJOR STERNAL
132.1
Origin
132.1.1 Sternum
to 7th rib, cartilages of true ribs and aponeurosis of external abdominal
oblique muscle
132.2
Insertion
132.2.1 Lateral
lip of the intertubercular sulcus of the humerus
132.2.2 Crest
of greater tubercle
132.3
Action
132.3.1 Flexion,
adduction ,medial rotation and horizontal flexion of the humerus at the
shoulder. Also extends flexed humerus. Through its action on the humerus it
depresses, protracts and rotates scapula downwards
132.4
Nerve Supply
132.4.1 Lateral
and medial pectoral, C7, 8, T1
132.5
Synergists
132.5.1 Latissimus
dorsi, subscapularis, teres major
132.6
Category
132.6.1
132.7
View
132.7.1
Anterior View
133
PECTORALIS MINOR
133.1
Origin
133.1.1 Anterior
surfaces of 3rd, 4th and 5th ribs near the costal cartilages
133.2
Insertion
133.2.1 Coracoid
process of the scapula
133.3
Action
133.3.1 Depresses
scapula and rotates scapula downward. Im- portant anterior shoulder stabilizer
133.3.2 Reversed
origin-insertion action
133.3.2.1 When
the scapula is fixed, it aids in rib elevation in forced inspiration
133.4
Nerve Supply
133.4.1 Medial
pectoral nerve from brachial plexus, C6, 7, 8
133.5
Synergists
133.5.1 Pectoralis
major, serratus anterior
133.6
Category
133.6.1
133.7
View
133.7.1
Anterior View
134
PERONEUS BREVIS
Back Table of Contents References
134.1
Word Count
134.1.1 1378/250=5.512
134.2
Word Derivation and Pronunciation
134.3
Pronunciation
134.3.1.1 PERONEUS BREVIS-PeRO’ NE US BREVIS
134.3.1.2 Pronunciation Key
134.3.2
Etymology
134.3.2.1 peróne=fibula
134.3.2.2 brevis=brief or
short
134.3.3 Naming
134.3.3.1 This muscle is
named because of its location on the fibula
(perone means fibula) and size (brevis means
short).
134.4
Category
134.4.1 Foot & Toes (Lateral
Peroneal Compartment)
134.5
View
134.5.1
Lateral and Plantar View
134.6
Attachments
134.6.1 Origin
134.6.1.1 Distal
2/3 of the lateral surface of the body of fibula
134.6.1.2 Adjacent
intermuscular septa
134.6.2 Insertion
134.6.2.1 Tuberosity
on lateral side of base of 5th metatarsal
134.7
Anatomical Markings & Structures
134.7.1 Fibula
134.7.2 Intermuscular
Septa
134.7.2.1 Definition
134.7.2.2 Illustrations
134.7.2.2.1
Superficial Muscles and
Tendons of the Right Lower Thigh and Leg, Lateral View
134.7.2.2.2
Muscles of the Anterior
Compartment of the Leg
134.7.2.2.3
Nerves and Arteries of the
Anterior and Lateral Compartments of the Leg
134.7.2.2.4
Muscles of the Lateral
Compartment of the Leg
134.7.3 Metatarsals
134.7.3.1 Tuberosity
134.7.3.2 Metatarsus
134.7.3.3 Bones of the right Foot,
Dorsal View
134.7.3.4 The Fifth Metatarsal Bone
134.7.3.5 Metatarsals
134.8
Joints
134.9
Tibiofibular (Inferior or
Distal)
134.9.1 Talocrural (Ankle) Joint
(ta’’lo-krōōr’al)
134.9.2 Subtalar/Talocalcaneal
(ta’’lo-kal-ka-ne-al)
134.9.3 Calcaneocuboid
134.9.4 5th Tarsometatarsal
134.10
Action
134.10.1 Eversion
(Foot-Ankle)
134.10.2 Plantar
flexion (Foot-Ankle)
134.10.3 Gives
lateral stability to the ankle
134.10.3.1
Reversed Origin-Insertion &
change of action
134.10.3.1.1 When the foot is stabilized,
as in standing, the peroneus longus and brevis stabilize the leg on the foot.
134.10.3.1.2 They are synergistic to the
gastrocnemius and soleus in extending the tibia and fibula at the ankle when in
the standing position.
134.11
Nerve Supply
134.11.1 Nerve
134.11.1.1
Superficial Peroneal
134.11.2 Roots
134.11.2.1
L4
134.11.2.2
L5
134.11.2.3
S1
134.11.2.4
S2
134.12
Muscle and Lever Type
134.12.1 Muscle Type
134.12.1.1
Unknown
134.12.2 Lever Type
134.12.2.1
Third
Class Levers
134.13
Synergists
134.13.1 Plantar Flexion
134.13.1.1
Peroneus Longus
134.13.1.2
Gastrocnemius
134.13.1.3
Soleus
134.13.1.4
Plantaris
134.13.1.5
Flexor Digitorum Longus
134.13.1.6
Flexor Hallucis Longus
134.13.1.7
Tibialis Posterior
134.13.2 Eversion/Pronation
134.13.2.1
Peroneus Longus
134.13.2.2
Peroneus Tertius
134.13.2.3
Extensor Digitorum Longus
134.13.3 Lateral Ankle
Stabilization
134.13.3.1
Peroneus Longus
134.13.4 Fixators
134.13.4.1
None
134.14
Antagonists
134.14.1 Inversion/Supination
134.14.1.1
Tibialis Anterior
134.14.1.2
Tibialis Posterior
134.14.1.3
Extensor Hallucis Longus
134.14.1.4
Gastrocnemius
134.14.1.5
Soleus
134.14.1.6
Flexor Digitorum Longus
134.14.1.7
Flexor Hallucis Longus
134.14.2 Dorsiflexion
134.14.2.1
Tibialis Anterior
134.14.2.2
Extensor Digitorum Longus
134.14.2.3
Extensor Hallucis Longus
134.14.2.4
Peroneus Tertius
134.14.3 Medial Ankle
Stabilization
134.14.3.1
Flexor Digitorum Longus
134.14.3.2
Flexor Hallucis Longus
134.14.3.3
Tibialis Posterior
134.15
Muscle Tests
134.15.1 Peroneus Longus & Brevis
134.16
Trigger Points
134.16.1 Peroneus Brevis, Peroneus
Longus, & Peroneus Tertius
134.17
Organ Reflexes (Neurolymphatic & Neurovascular)
134.17.1 Bladder
134.17.2 Illustrations
134.18
Acupressure/Acupuncture Theory
134.18.1 Organs
134.18.1.1
Kidneys & Bladder
134.18.2 Channels
Discussion
134.18.2.1
Bladder
134.18.3 Channel
134.18.3.1
Bladder Illustration
134.18.4 Command Points
134.18.4.1
Bladder
134.19
Nutritional
134.19.1 Calcium
134.19.2 Vitamin B Complex
134.19.3 Avoid Oxalic Acid
Foods
134.20
Musculoskeletal Pathology
134.20.1 Peroneal
Tendonitis/ Tenosynovitis
134.20.2 Peroneal Tendon Dislocation/Subluxation
134.20.3 Ankle Varus
134.20.4 Ankle Valgus
134.21 Orthopaedic Tests
134.21.1 Foot Position
134.21.2 Foot Arches
134.21.3 Ankle Circumference
134.21.4 Tenderness Ankle/Foot
134.21.5 Ankle Range of Motion
134.21.6 Foot Condition
134.22
Musculoskeletal Examination
134.22.1 Peroneal Tubercle
134.22.2 Peroneus Longus & Brevis
Tendon
134.22.3 Peroneus Longus & Brevis
Muscle Test
134.23
Stretching
134.23.1 Stretching Concepts
134.23.2 Stretching Individual Muscle
Discussion
134.23.3 Stretching Muscle
Illustration
134.24
Posture
134.24.1
Feet & Knees
134.24.2
Knees & Legs
134.25 Massage Routines
134.25.1 Deep Tissue
134.25.1.1
Lateral
Leg Separation
134.26
Exercise
134.26.1 Peroneus Longus &
Brevis-Resistance Exercise
134.26.2 Peroneus Longus & Brevis-
Biomechanics
134.27
Range of Motion Exercise (ROM)
134.27.1 Ankle: dorsiflexion
134.27.2 Ankle: plantarflexion
134.27.3 Subtalar (lower ankle) joint:
inversion and eversion
134.27.4 Transverse tarsal joint:
supination and pronation
134.28
Peripheral Joint Mobilization
134.28.1 Distal tibiofibular
articulation-Anterior (ventral) or posterior (dorsal) glide
134.28.2 Talocrural (upper ankle
joint) (Convex talus articulates with the concave mortice made up of the tibia
and fibula)
134.28.3 Subtalar (talocalcaneal)
joint, posterior compartment
134.28.4 Intertarsal joints and
tarsometatarsal joints
134.29
Surgical Anatomy
134.29.1 Anterior Ankle
134.29.2 Posterior Ankle
134.29.3 Lower Leg Posterior
134.29.4 Lower Leg Posterior
134.29.5 Sole of Foot 3rd Layer
134.29.6 Anterior Foot Deep
134.29.7 Anterior Ankle Tibiofibular
Joint
134.29.8 Medial Ankle Joint
134.29.9 Posterior Ankle Tibiofibular
Joint
134.29.10
Lateral Ankle Joint
134.29.11
Superior Tarsus
134.29.12
Inferior Tarsus
134.30
Miscellaneous Illustrations
134.30.1
Tissue Organization
134.30.1.1
Synovial (Mucous) Sheaths of the Tendons & Retinaculum
(Ligaments) Around the Ankle (Lateral & Medial)
134.30.1.2
Tendons at
the Ankle Region Dorsolateral View (Right Foot)
134.30.1.3
Tendons of the Peroneus Longus and Tibialis Anterior Muscle
134.30.2 Skeletal
System-Appendicular Skeleton
134.30.2.1
Tibiofibular
Union and Interosseous Membrane (Right Leg)
134.30.2.2
Right Tibia Posterior View
134.30.2.3
Bones of the right Foot, Dorsal View
134.30.2.4
Bones of the Right Foot Plantar View
134.30.2.5
Right Foot Dorsal/Plantar
134.30.2.6
Left Talus
134.30.2.7 Calcaneus
134.30.2.8
Navicular and Cuboid Bones
134.30.2.9
1st, 2nd, and 3rd Cuneiform
Bones
134.30.2.10
Metatarsals
134.30.3
Articulations
134.30.3.1
Right Foot Lateral & Medial Ligaments
134.30.3.2
Plantar Ligaments & Joints
134.30.3.3
Right Foot Synovial Joint Cavities
134.30.3.4
Ligaments
of the Ankle and Foot Dorsolateral View (Right Foot)
134.30.3.5
Ligaments
of the Ankle and Foot Medial View (Right Foot)
134.30.3.6
Intertarsal
and Tarsometatarsal Joints (Horizontal Section of the Right Foot)
134.30.3.7
Talocalcaneonavicular
Joint (Viewed from above) Right
134.30.3.8
Ankle Joint (Talocrural) Viewed from Behind (Right Foot)
134.30.3.9
Ligaments
on the Plantar Surface of the Right Foot (Superficial)
134.30.3.10
Plantar
Calcaneonavicular Ligament and the Insertions of three Tendons (Right Foot)
134.30.3.11
Synovial Joint Types
134.30.3.12
Generalized Synovial Joint Capsule Frontal Section
134.31
Discussion (Gray)
134.31.1 The Peroneus brevis
lies under cover of the Peroneus longus, and is a shorter and smaller muscle.
It arises from the lower two-thirds of the lateral surface of the body of the
fibula; medial to the Peroneus longus; and from the intermuscular septa
separating it from the adjacent muscles on the front and back of the leg. The
fibers pass vertically downward, and end in a tendon, which runs behind the
lateral malleolus along with but in front of that of the preceding muscle, the
two tendons being enclosed in the same compartment, and lubricated by a common
mucous sheath. It then runs forward on the lateral side of the calcaneus, above
the trochlear process and the tendon of the Peroneus longus, and is inserted
into the tuberosity at the base of the fifth metatarsal bone, on its lateral
side.
134.31.2 On the lateral surface of the calcaneus the
tendons of the Peronei longus and brevis occupy separate Osseo aponeurotic
canals formed by the calcaneus and the Perineal retinacula; each tendon is
enveloped by a forward prolongation of the common mucous sheath.
134.31.3 Variations
134.31.3.1
Fusion of the two peronei is rare. A slip from the Peroneus
longus to the base of the third, fourth or fifth metatarsal bone, or to the
Adductor hallucis is occasionally seen.
134.31.3.2
Peroneus
accessorius, origin from the fibula between the longus and brevis, joins the
tendon of the longus in the sole of the foot.
36
134.31.3.3
Peroneus quinti
digiti, rare, origin lower fourth of the fibula under the brevis, insertion
into the Extensor aponeurosis of the little toe. More common as a slip of the
tendon of the Peronæus brevis. 37
134.31.3.4
Peronæus quartus, 13
per cent. (Gruber), origin back of fibula between the brevis and the Flexor
hallucis, insertion into the peroneal spine of the calcaneum, (peroneocalcaneus
externum), or less frequently into the tuberosity of the cuboid
(peroneocuboideus). 38
134.31.4 Nerves.
134.31.4.1
The Peronei longus
and brevis are supplied by the fourth and fifth lumbar and first sacral nerves
through the superficial peroneal nerve.
134.31.5 Actions.
134.31.5.1
The Peronei longus and brevis extend the foot upon the leg,
in conjunction with the Tibialis posterior, antagonizing the Tibialis anterior
and Peroneus tertius, which are flexors of the foot. The Peroneus longus also
everts the sole of the foot, and from the oblique direction of the tendon
across the sole of the foot is an important agent in the maintenance of the
transverse arch. Taking their fixed points below, the Peronei serve to steady
the leg upon the foot. This is especially the case in standing upon one leg,
when the tendency of the super incumbent weight is to throw the leg medialward;
the Peroneus longus overcomes this tendency by drawing on the lateral side of
the leg.
134.31.6 Discussion
134.31.6.1
http://www.bartleby.com/107/129.html
134.31.7 Illustration
134.31.7.1
http://www.bartleby.com/107/illus439.html
134.31.7.2
http://www.bartleby.com/107/illus440.html
134.31.7.3
http://www.med.umich.edu/rad/muscskel/mskus/images/188/188_lat.html
134.31.8 Research
134.31.8.1
http://www.aofas.org/i4a/pages/index.cfm?pageid=3984
134.31.8.2
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=164378
134.31.8.3
http://www.aaos.org/wordhtml/anmt2005/poster/p179.htm
134.31.8.4
http://www.neurology.org/cgi/content/abstract/55/5/636
134.31.8.5
http://bjsm.bmjjournals.com/cgi/content/abstract/36/1/65
134.31.8.6
http://www.emedicine.com/sports/topic98.htm
134.31.8.7
http://www.straws.com/a_perote.htm
134.32
Practice Questions & Answers
134.32.1 Peroneus Brevis Practice
Questions
134.32.2 Peroneus Brevis Answers to
Practice Test
135
PERONEUS LONGUS
Back Table of Contents References
135.1
Word Derivation and Pronunciation
135.2
Pronunciation
135.2.1.1 PERONEUS LONGUS-
135.2.1.2 Pronunciation Key
135.2.2 Etymology
135.2.2.1 perone=fibula
135.2.2.2 longus=long
135.3
START
135.4
Attachment
135.4.1 Origin
135.4.1.1 Lateral condyle of
tibia
135.4.1.2 Head
and proximal 2/3 of lateral surface of fibula
135.4.1.3 Intermuscular
septa and adjacent fascia
135.4.2 Insertion
135.4.2.1 Lateral
margin of plantar surface of 1st cuneiform
135.4.2.2 Base
of 1st metatarsal
135.5
Joints
135.6
Ankle (Talocrural)
135.7
Tibiofibular
135.8
Metatarsal/Tarsal
135.9
Action
135.9.1 Eversion
(Foot-Ankle)
135.9.2 Plantar
flexion (Foot-Ankle)
135.9.3 Gives
lateral stability to the ankle
135.9.4 Reversed
Origin-Insertion & change of action
135.9.4.1 When the foot is
stabilized, as in standing, the peroneus longus and brevis stabilize the leg on
the foot.
135.9.4.2 They are
synergistic to the gastrocnemius and soleus in extending the tibia and fibula
at the ankle when in the standing position.
135.10
Nerve Supply
135.10.1 Nerve
135.10.1.1
Superficial peroneal
135.10.2 Roots
135.10.2.1
L4
135.10.2.2
L5
135.10.2.3
S1
135.10.2.4
S2
135.11
Synergists
135.11.1 Gastrocnemius
135.11.2 Soleus (plantar flexion)
135.11.3 Peroneus
brevis (Eversion)
135.11.4 Peroneus
Tertius (Eversion)
135.12
Muscle Tests
135.12.1
PERONEUS
LONGUS & BREVIS
135.13
Trigger Points
135.13.1
PERONEUS BREVIS, PERONEUS
LONGUS, & PERONEUS TERTIUS
135.14
Organ Reflexes (Neurolymphatic & Neurovascular)
135.14.1 Bladder
135.14.2 Illustrations
135.15
Acupressure/Acupuncture Theory
135.15.1 Organs
135.15.1.1
Kidneys & Bladder
135.15.2 Channels
Discussion
135.15.2.1
Bladder
135.15.3 Channel
135.15.3.1
Bladder Illustration
135.15.4 Command Points
135.15.4.1
Bladder
135.16
Nutritional
135.16.1 Calcium
135.16.2 Vitamin B Complex
135.16.3 Avoid Oxalic Acid
Foods
135.17
Discussion (Gray)
135.17.1 The Peronæus
longus is situated at the upper part of the lateral side of the leg, and is the
more superficial of the two muscles. It arises from the head and upper
two-thirds of the lateral surface of the body of the fibula, from the deep
surface of the fascia, and from the intermuscular septa between it and the
muscles on the front and back of the leg; occasionally also by a few fibers
from the lateral condyle of the tibia. Between its attachments to the head and
to the body of the fibula there is a gap through which the common peroneal
nerve passes to the front of the leg. It ends in a long tendon, which runs
behind the lateral malleolus, in a groove common to it and the tendon of the
Peronæus brevis, behind which it lies; the groove is converted into a canal by
the superior peroneal retinaculum, and the tendons in it are contained in a
common mucous sheath. The tendon then extends obliquely forward across the
lateral side of the calcaneus, below the trochlear process, and the tendon of the
Peronæus brevis, and under cover of the inferior peroneal retinaculum. It
crosses the lateral side of the cuboid, and then runs on the under surface of
that bone in a groove which is converted into a canal by the long plantar
ligament; the tendon then crosses the sole of the foot obliquely, and is
inserted into the lateral side of the base of the first metatarsal bone and the
lateral side of the first cuneiform. Occasionally it sends a slip to the base
of the second metatarsal bone. The tendon changes its direction at two points:
first, behind the lateral malleolus; secondly, on the cuboid bone; in both of
these situations the tendon is thickened, and, in the latter, a sesamoid
fibrocartilage (sometimes a bone), is usually developed in its substance.
135.17.2 Discussion
135.17.2.1
http://www.bartleby.com/107/129.html
135.17.3 Illustration
135.17.3.1
http://www.bartleby.com/107/illus439.html
135.17.3.2
http://www.bartleby.com/107/illus440.html
135.18
Category
135.18.1 Foot & Toes (Lateral
Peroneal Compartment)
135.19
View
135.19.1 Lateral
and Plantar View
136
PERONEUS TERTIUS
Back Table of Contents References
136.1
Attachments
136.1.1 Origin
136.1.1.1 Distal
1/3 of the anterior surface of the fibula
136.1.1.2 Interosseous
membrane
136.1.1.3 Adjacent
intermuscular septum
136.1.2 Insertion
136.1.2.1 Dorsal
surface of the base of the 5th metatarsal
136.2
Action
136.2.1 Dorsiflexes
and everts the foot at the ankle
136.3
Nerve Supply
136.3.1 Nerve
136.3.1.1 Deep
peroneal
136.3.2
Roots
136.3.2.1 L5
136.3.2.2 S1
136.4
Synergists
136.4.1 Extensor
digitorum longus for dorsiflexion
136.4.2 Peroneus
longus and brevis (for eversion)
136.5
Muscle Tests
136.5.1
136.6
Trigger Points
136.6.1
136.7
Discussion (Gray)
136.7.1 The Peronæus tertius
is a part of the Extensor digitorum longus, and might be described as its fifth
tendon. The fibers belonging to this tendon arise from the lower third or more
of the anterior surface of the fibula; from the lower part of the interosseous
membrane; and from an intermuscular septum between it and the Peronæus brevis.
The tendon, after passing under the transverse and cruciate crural ligaments in
the same canal as the Extensor digitorum longus, is inserted into the dorsal
surface of the base of the metatarsal bone of the little toe. This muscle is
sometimes wanting. 9
136.7.2
136.7.3 Nerves.—These
muscles are supplied by the fourth and fifth lumbar and first sacral nerves
through the deep peroneal nerve. 10
136.7.4
136.7.5 Actions.—The
Tibialis anterior and Peronæus tertius are the direct flexors of the foot at
the ankle-joint; the former muscle, when acting in conjunction with the
Tibialis posterior, raises the medial border of the foot, i. e., inverts the
foot; and the latter, acting with the Peronæi brevis and longus, raises the
lateral border of the foot, i. e., everts the foot. The Extensor digitorum
longus and Extensor hallucis longus extend the phalanges of the toes, and,
continuing their action, flex the foot upon the leg. Taking their fixed points
from below, in the erect posture, all these muscles serve to fix the bones of
the leg in the perpendicular position, and give increased strength to the
ankle-joint.
136.7.6 Discussion
136.7.6.1 http://www.bartleby.com/107/129.html
136.7.7 Illustration
136.7.7.1 http://www.bartleby.com/107/illus437.html
136.7.7.2 http://www.bartleby.com/107/illus440.html
136.8
Category
136.8.1 Foot & Toes (Anterior
Compartment)
136.9
View
136.9.1
Lateral View
137
PIRIFORMIS (1
of 6 Deep Lateral Rotators of Femur)
137.1
Origin
137.1.1 Anterior
surface of sacrum between and lateral to anterior sacral foramina, capsule of
sacroiliac articulation, margin of the greater sciatic foramen, and
sacrotuberous ligament
137.2
Insertion
137.2.1 Superior
border of greater trochanter of femur
137.3
Action
137.3.1 Rotates
thigh laterally and abducts the flexed thigh at the hip
137.4
Nerve Supply
137.4.1 Sacral
plexus, L5, S1, 2
137.5
Synergists
137.5.1 Superior
and inferior gemelli, quadratus femoris, internal and external obturators
137.6
Category
137.6.1
137.7
View
137.7.1
Posterior View
138
PLANTAR INTEROSSEI (FOOT)
Back Table of Contents References
138.1
Attachments
138.1.1 Origin
138.1.1.1 There
are 3 plantar Interossei arising from the bases and medial plantar surfaces of
the 3rd, 4th and 5th metatarsal bones
138.1.2 Insertion
138.1.2.1 Medial
sides of the bases of the proximal phalanges of the same toes and into the
extensor expansion
138.2
Action
138.2.1 Adducts
the 3rd, 4th and 5th toes toward the axis of the 2nd toe
138.2.2 Flex
the proximal and extend the distal phalanges
138.3
Nerve Supply
138.3.1 Nerve
138.3.1.1 Lateral
plantar
138.3.2 Roots
138.3.2.1 S2
138.3.2.2 S3
138.4
Synergists
138.4.1 Dorsal
Interossei
138.5
Muscle Tests
138.5.1
138.6
Trigger Points
138.6.1
138.7
Discussion (Gray)
138.7.1 The Interossei
plantares (Plantar interossei) (Fig. 447), three in number, lie beneath rather
than between the metatarsal bones, and each is connected with but one
metatarsal bone. They arise from the bases and medial sides of the bodies of
the third, fourth, and fifth metatarsal bones, and are inserted into the medial
sides of the bases of the first phalanges of the same toes, and into the
aponeuroses of the tendons of the Extensor digitorum longus. 31
138.7.2 Nerves.—The Flexor
digitorum brevis, the Flexor hallucis brevis, the Abductor hallucis, and the
first Lumbricalis are supplied by the medial plantar nerve; all the other
muscles in the sole of the foot by the lateral plantar. The first Interosseous
dorsalis frequently receives an extra filament from the medial branch of the
deep peroneal nerve on the dorsum of the foot, and the second Interosseous
dorsalis a twig from the lateral branch of the same nerve. 32
138.7.3 Actions.—All the
muscles of the foot act upon the toes, and may be grouped as abductors, adductors,
flexors, or extensors. The abductors are the Interossei dorsales, the Abductor
hallucis, and the Abductor digiti quinti. The Interossei dorsales are abductors
from an imaginary line passing through the axis of the second toe, so that the
first muscle draws the second toe medialward, toward the great toe, the second
muscle draws the same toe lateralward, and the third and fourth draw the third
and fourth toes in the same direction. Like the Interossei in the hand, each
assists in flexing the first phalanx and extending the second and third
phalanges. The Abductor hallucis abducts the great toe from the second, and
also flexes its proximal phalanx. In the same way the action of the Abductor
digiti quinti is twofold, as an abductor of this toe from the fourth, and also
as a flexor of its proximal phalanx. The adductors are the Interossei plantares
and the Adductor hallucis. The Interossei plantares adduct the third, fourth,
and fifth toes toward the imaginary line passing through the second toe, and by
means of their insertions into the aponeuroses of the Extensor tendons they
assist in flexing the proximal phalanges and extending the middle and terminal
phalanges. The oblique head of the Adductor hallucis is chiefly concerned in
adducting the great toe toward the second one, but also assists in flexing this
toe; the transverse head approximates all the toes and thus increases the curve
of the transverse arch of the metatarsus. The flexors are the Flexor digitorum
brevis, the Quadratus plantæ, the Flexor hallucis brevis, the Flexor digiti
quinti brevis, and the Lumbricales. The Flexor digitorum brevis flexes the
second phalanges upon the first, and, continuing its action, flexes the first
phalanges also, and brings the toes together. The Quadratus plantæ assists the
Flexor digitorum longus and converts the oblique pull of the tendons of that
muscle into a direct backward pull upon the toes. The Flexor digiti quinti
brevis flexes the little toe and draws its metatarsal bone downward and
medialward. The Lumbricales, like the corresponding muscles in the hand, assist
in flexing the proximal phalanges, and by their insertions into the tendons of
the Extensor digitorum longus aid that muscle in straightening the middle and
terminal phalanges. The Extensor digitorum brevis extends the first phalanx of
the great toe and assists the long Extensor in extending the next three toes,
and at the same time gives to the toes a lateral direction when they are
extended.
138.7.4 Discussion
138.7.4.1 http://www.bartleby.com/107/131.html
138.7.5 Illustration
138.7.5.1 http://www.bartleby.com/107/illus447.html
138.8
Category
138.8.1 Intrinsic Foot (Plantar 4th
Deep Layer)
138.9
View
138.9.1
Plantar View (4th Plantar Layer)
139
PLANTARIS
Back Table of Contents References
139.1
Attachments
139.1.1 Origin
139.1.1.1 Lower
part of lateral supracondylar line of femur
139.1.1.2 Oblique
popliteal ligament of the knee joint
139.1.2 Insertion
139.1.2.1 The
posterior part of the calcaneus medial to the Achilles tendon
139.2
Action
139.2.1 Plantar
flexion (Foot=ankle)
139.2.2 Inversion
(Foot=ankle) at the ankle
139.2.3 Flexes
the leg at the knee
139.3
Nerve Supply
139.3.1 Nerve
139.3.1.1 Tibial
nerve
139.3.2 Roots
139.3.2.1 L4
139.3.2.2 L5
139.3.2.3
S1
139.3.2.4 S2
139.4
Synergists
139.4.1 Gastrocnemius
139.4.2 Soleus
139.4.3 Tibialis
posterior
139.4.4 Peroneus
longus
139.4.5 Peroneus
brevis
139.4.6 Flexor
hallucis longus
139.4.7 Flexor
digitorum longus
139.5
Muscle Tests
139.5.1
139.6
Trigger Points
139.6.1
139.7
Discussion (Gray)
139.7.1 The Plantaris is placed
between the Gastrocnemius and Soleus. It arises from the lower part of the
lateral prolongation of the linea aspera, and from the oblique popliteal
ligament of the knee-joint. It forms a small fusiform belly, from 7 to 10 cm.
long, ending in a long slender tendon which crosses obliquely between the two
muscles of the calf, and runs along the medial border of the tendo calcaneus,
to be inserted with it into the posterior part of the calcaneus. This muscle is
sometimes double, and at other times wanting. Occasionally, its tendon is lost
in the laciniate ligament, or in the fascia of the leg. 19
139.7.2
139.7.3 Nerves.—The
Gastrocnemius and Soleus are supplied by the first and second sacral nerves,
and the Plantaris by the fourth and fifth lumbar and first sacral nerves,
through the tibial nerve. 20
139.7.4
139.7.5 Actions.—The
muscles of the calf are the chief extensors of the foot at the ankle-joint.
They possess considerable power, and are constantly called into use in
standing, walking, dancing, and leaping; hence the large size they usually
present. In walking, these muscles raise the heel from the ground; the body
being thus supported on the raised foot, the opposite limb can be carried
forward. In standing, the Soleus, taking its fixed point from below, steadies
the leg upon the foot and prevents the body from falling forward. The
Gastrocnemius, acting from below, serves to flex the femur upon the tibia,
assisted by the Popliteus. The Plantaris is the rudiment of a large muscle
which in some of the lower animals is continued over the calcaneus to be
inserted into the plantar aponeurosis. In man it is an accessory to the
Gastrocnemius, extending the ankle if the foot be free, or bending the knee if
the foot be fixed.
139.7.6 Discussion
139.7.6.1 http://www.bartleby.com/107/129.html
139.7.7 Illustration
139.7.7.1 http://www.bartleby.com/107/illus438.html
139.7.7.2 http://www.bartleby.com/107/illus440.html
139.8
Category
139.8.1 Foot & Toes (Posterior
Superficial Compartment)
139.9
View
139.9.1
Posterior View
140
PLATYSMA
140.1
Origin
140.1.1 Broad. fascial.sheet over the .~pper
parts of the pectoralis major and antenor portion of the deltbld
140.2
Insertion
140.2.1 Anterior Fibers
140.2.1.1 Interlace across the midline
inferoposterior to symphysis menti
140.2.2 Intermediate Fibers
140.2.2.1 Pars mandibularis lthe lower border of the body of the
mandible. Pars abialis, deep t.o depressor angu1i oris to the
lateral half of the lower lip
140.2.3 Posterior Fibers
140.2.3.1 Pars modiolaris, the skin and
subcutaneous tissue blending with the muscles at the modiolus near the buccal
ang1e
140.3
Action
140.3.1 Anterior Fibers
140.3.1.1 Assist mandibular depression
140.3.2 Intermediate Fibers
140.3.2.1 Pars labialis depress the lower lip
140.3.3 Posterior Fibers
140.3.3.1 Pars modiolaris, depress the buccal
angle
140.4
Nerve Supply
140.4.1 Cervical branch of the facial nerve
(VII)
140.5
Arterial
Supply
140.5.1 Submental and inferiouabial branches of
the facial
arteries, mental branch of the inferior alveolar artery, superior !ind inferior
l~ryngeal arteries, and perforating branclies of the Internal thoracic artery
140.6
Synergists
140.6.1 Depressor anguli oris
140.7
Antagonist
140.7.1 Levator anguli oris
140.8
Category
140.8.1
140.9
Note
140.9.1
(Denotes
modiolus)
141
POPLITEUS
Back Table of Contents References
141.1
Attachments
141.1.1 Origin
141.1.1.1 Lateral
condyle of femur
141.1.1.2 Outer
margin of lateral meniscus
141.1.1.3 Arcuate
popliteal ligament and capsule of knee joint
141.1.2 Insertion
141.1.2.1 Posterior
surface of tibia above Soleal line
141.2
Action
141.2.1 Rotates
the tibia medially on the femur (depending on fixation)
141.2.2 Rotates
the femur laterally on the tibia (depending on fixation)
141.2.3 Withdraws
the meniscus during flexion
141.2.4 Provides
rotatory stability to the femur on the tibia
141.2.5 Brings
the knee out of the position of full extension
141.2.6 Helps
with posterior stability of the knee
141.3
Nerve Supply
141.3.1 Nerve
141.3.1.1 Tibial
141.3.2 Roots
141.3.2.1 L4
141.3.2.2 L5
141.3.2.3 S1
141.4
Synergists
141.4.1
141.5
Muscle Tests
141.5.1
141.6
Trigger Points
141.6.1
141.7
Discussion (Gray)
141.7.1 The Popliteus is a
thin, flat, triangular muscle, which forms the lower part of the floor of the
popliteal fossa. It arises by a strong tendon about 2.5 cm. long, from a
depression at the anterior part of the groove on the lateral condyle of the
femur, and to a small extent from the oblique popliteal ligament of the
knee-joint; and is inserted into the medial two-thirds of the triangular
surface above the popliteal line on the posterior surface of the body of the
tibia, and into the tendinous expansion covering the surface of the
muscle. 23
141.7.2
141.7.3 Variations.—Additional
head from the sesamoid bone in the outer head of the Gastrocnemius. Popliteus
minor, rare, origin from femur on the inner side of the Plantaris, insertion into
the posterior ligament of the knee-joint. Peroneotibialis, 14 per cent., origin
inner side of the head of the fibula, insertion into the upper end of the
oblique line of the tibia, it lies beneath the Popliteus.
141.7.4 Discussion
141.7.4.1 http://www.bartleby.com/107/129.html
141.7.5 Illustration
141.7.5.1 http://www.bartleby.com/107/illus439.html
141.7.5.2 http://www.bartleby.com/107/illus440.html
141.8
Category
141.8.1 Foot & Toes (Posterior
Deep Compartment)
141.9
View
141.9.1 Posterior
View
142
POSTERIOR CRICOARYTENOID
142.1
Origin
142.1.1 Posterior surface of the cricoid
lamina, the inferomedial aspect of the depression present to the side of the
midline
142.2
Insertion
142.2.1 The apex of the arytenoid muscular
process, just medial to the lateral cricoarytenoid's attachment
142.3
Action
142.3.1 Rotates the a~enoid cartilages
laterally at the cricoarytenoid joints. The only muscle to aDduct the vocal
cords. This muscle alSo tenses the vocal cords
142.4
Nerve Supply
142.4.1 Recurrent laryngeal branch of the vagus
nerve (X)
142.5
Arterial
Supply
142.5.1 SuRerior laryngeal branch of the
suRerior thyro!d artery and the iliferior laryngeal branch of the inferior
thyrOId artery
142.6
Synergists
142.6.1 For glottis deviation
142.6.1.1 None
142.6.2 For regulating tension of vocal folds
142.6.2.1 Cricothyroid
142.7
Antagonists
142.7.1 For glottic deviation
142.7.1.1 Lateral cricoarytenoids, oblique and
transverse arytenoids
142.7.2 For regulating tension in vocal folds
142.7.2.1 Thyroarytenoids and vocalis
142.8
Category
142.8.1
143
PROCERUS
143.1
Origin
143.1.1 The facial aponeurosis covering the
lower part of the nasal bone and lateral nasaf cartilage
143.2
Insertion
143.2.1 Superficial fascia between the eyebrows
and continuous with frontalis
143.3
Action
143.3.1 Depresses the medial end of the eyebrow
143.4
Nerve Supply
143.4.1 Superior buccal branches of the facial
nerve (VII)
143.5
Arterial
Supply
143.5.1 Supratrochlear, supraorbital and dorsal
nasal branches of the ophthalmic artery
143.6
Synergists
143.6.1 Corrugator supercilii and orbicularis
oculi
143.7
Antagonist
143.7.1 Frontalis
143.8
Category
143.8.1
144
PRONATOR QUADRATUS
144.1
Origin
144.1.1 Distal
1/4 of the anterior surface of the ulna
144.2
Insertion
144.2.1 Distal
1/4 of the anterior surface of the radius. ACTION: Pronates the forearm
144.3
Action
144.3.1
144.4
Nerve Supply
144.4.1 Anterior
interosseous branch of median nerve, C8, T1
144.5
Synergists
144.5.1 Pronator
teres
144.6
Category
144.6.1
144.7
View
144.7.1
Anterior View
145
PRONATOR TERES
145.1
Origin
145.1.1 Humeral
head
145.1.1.1 Common
flexor tendon from medial epicon- dyle of humerus and common flexor tendon
145.1.2 Ulnar
head
145.1.2.1 Medial
side of coronoid process of ulna
145.2
Insertion
145.2.1 Middle
1/3 of lateral surface of radius
145.3
Action
145.3.1 Pronation
of forearm and flexion of forearm at the elbow
145.4
Nerve Supply
145.4.1 Median,
C6, 7
145.5
Synergists
145.5.1 Pronator
quadratus
145.6
Category
145.6.1
145.7
View
145.7.1
Anterior View
146
PSOAS MAJOR
146.1
Origin
146.1.1 Anterior
surfaces of transverse processes. Lateral borders of vertebral bodies and
corresponding intervertebral discs of T12 - L5
146.2
Insertion
146.2.1 Lesser
trochanter of femur and for short distance below along medial border of the
shaft
146.3
Action
146.3.1 Flexion
of the thigh at the hip. Minimal action in lateral rotation of the thigh
146.3.2 REVERSED
ORIGIN-INSERTION ACTION
146.3.2.1 When
the thigh is fixed, the psoas muscle pulls on the vertebrae and flexes the
spine and pelvis on the thigh (sit up)
146.4
Nerve Supply
146.4.1 Lumbar
plexus, L1, 2, 3
146.5
Synergists
146.5.1 Iliacus,
adductor brevis, adductor longus, adductor magnus, rectus femoris
146.6
Category
146.6.1
146.7
View
146.7.1
Anterior View
147
PSOAS MINOR
147.1
Origin
147.1.1
147.2
Insertion
147.2.1
147.3
Action
147.3.1
147.4
Nerve Supply
147.4.1
147.5
Synergists
147.5.1
147.6
Category
147.6.1
148
PYRAMIDALIS
148.1
Origin
148.1.1 Anterior
aspect of the symphysis pubis and pubic bone
148.2
Insertion
148.2.1 Linea
alba, midway between the umbilicus and pubis
148.3
Action
148.3.1 Compresses
the abdomen, supports abdominal viscera, tenses the linea alba and is active in
forced expiration
148.4
Nerve Supply
148.4.1 Subcostal
nerve, T12
148.5
Synergists
148.5.1 Rectus
abdominis, external abdominal oblique, internal abdominal oblique, transversus
abdominis
148.6
Category
148.6.1
148.7
View
148.7.1
Anterior View
149
QUADRATUS FEMORIS (1
of 6 Deep Lateral Rotators of the Femur)
149.1
Origin
149.1.1 Superior
aspect of the lateral border of the ischial tuberosity
149.2
Insertion
149.2.1 Superior
aspect of the quadrate line which extends downward from the intertrochanteric
crest of the femur
149.3
Action
149.3.1 Lateral
rotation of the femur at the hip
149.4
Nerve Supply
149.4.1 Sacral
plexus, L4, 5, S1
149.5
Synergists
149.5.1 Piriformis,
obturator externus, obturator internus, superior and inferior gemelli
149.6
Category
149.6.1
149.7
View
149.7.1
Posterior View
150
QUADRATUS LUMBORUM
150.1
Origin
150.1.1 Iliolumbar
ligament, posterior part of the iliac crest
150.2
Insertion
150.2.1 Inferior
border of the 12th rib and transverse proces- ses of the upper 4 lumbar
vertebrae
150.3
Action
150.3.1 Lateral
flexion of lumbar vertebral column; helps action of the diaphragm in
inspiration
150.4
Nerve Supply
150.4.1 Lumbar
plexus, T12, L1, 2, 3
150.5
Synergists
150.5.1 Internal
and external abdominal obliques, iliocos- talis lumborum, longissimus thoracis
and psoas major
150.6
Category
150.6.1
150.7
View
150.7.1
Posterior View
151
QUADRATUS PLANTAE
Back Table of Contents References
151.1
Word Derivation and Pronunciation
151.2
Pronunciation
151.2.1.1 QUADRATUS PLANTAE
151.2.1.1.1
None
151.2.1.2 Pronunciation Key
151.2.2 Etymology
151.2.2.1 Quad=Four
151.2.2.2 Planta=Sole of
foot
151.3
Attachments
151.3.1 Origin
151.3.1.1 Two
heads from the medial and lateral sides of the inferior surface of the
calcaneus
151.3.1.2 Medial
Head
151.3.1.2.1
Medial
surface of calcaneus
151.3.1.2.2
Medial
border of long plantar ligament
151.3.1.3 Lateral Head
151.3.1.3.1
Lateral
border of plantar surface of calcaneus
151.3.1.3.2
Lateral
border of long plantar ligament
151.3.2 Insertion
151.3.2.1 Lateral
border and dorsal and plantar surfaces of the tendon of the flexor digitorum
longus
151.4
Joints
151.5
Metatarsal/Tarsal
151.6
Action
151.6.1 Flexes
the 2nd -5th toes
151.6.2 Modifies
the line of pull of the flexor digitorum longus tendon
151.7
Nerve Supply
151.7.1 Nerve
151.7.1.1 Tibial
151.7.1.2 Lateral
plantar
151.7.2 Roots
151.7.2.1 S1
151.7.2.2 S2
151.7.2.3 S3
151.8
Synergists
151.8.1 Flexor
Digitorum Longus
151.8.2 Flexor
Digitorum Brevis
151.9
Muscle Tests
151.9.1 FLEXOR DIGITORUM LONGUS
& QUADRATUS PLANTAE
151.10
Trigger Points
151.10.1
QUADRATUS PLANTAE
151.11
Organ Reflexes
151.11.1 None
151.11.2 Illustrations
151.12
Acupressure/Acupuncture Theory
151.12.1 None
151.13
Nutritional
151.13.1 None
151.14
Discussion (Gray)
151.14.1 The Quadratus
plantæ (Flexor accessorius) is separated from the muscles of the first layer by
the lateral plantar vessels and nerve. It arises by two heads, which are
separated from each other by the long plantar ligament: the medial or larger
head is muscular, and is attached to the medial concave surface of the
calcaneus, below the groove which lodges the tendon of the Flexor hallucis
longus; the lateral head, flat and tendinous, arises from the lateral border of
the inferior surface of the calcaneus, in front of the lateral process of its
tuberosity, and from the long plantar ligament. The two portions join at an
acute angle, and end in a flattened band which is inserted into the lateral
margin and upper and under surfaces of the tendon of the Flexor digitorum
longus, forming a kind of groove, in which the tendon is lodged. It usually
sends slips to those tendons of the Flexor digitorum longus which pass to the
second, third, and fourth toes. 19
151.14.2 Variations.—Lateral
head often wanting; entire muscle absent. Variation in the number of digital
tendons to which fibers can be traced. Most frequent offsets are sent to the
second, third and fourth toes; in many cases to the fifth as well; occasionally
to two toes only.
151.14.3 Discussion
151.14.3.1
http://www.bartleby.com/107/131.html
151.14.4 Illustration
151.14.4.1
http://www.bartleby.com/107/illus444.html
151.15
Category
151.15.1 Intrinsic Foot (Plantar 2nd
Layer)
151.16
View
151.16.1 Plantar
View (2nd Plantar Layer)
152
RECTUS ABDOMINIS (4
Divisions as 1)
152.1
Origin
152.1.1 The
pubic crest and the symphysis pubis
152.2
Insertion
152.2.1 The
costal cartilages of the Sth, 6th and 7th ribs and the side of the xiphoid
process
152.3
Action
152.3.1 Flexion
and lateral flexion of the trunk. In standing position, supports organs
anteriorly, gives anterior support to lum- bar spine. With aid of gluteus
maximus and hamstrings keeps pelvis from going into anterior tilt, decreasing
lumbar lordosis
152.4
Nerve Supply
152.4.1 Ventral
rami of TS -12. The various levels of the rectus abdominis, superior, inferior
as well as those between in- scriptions receive nerve supply from different
levels. Therefore act independently as they influence each other
152.5
Synergists
152.5.1 Internal
and external oblique abdominals, pyramidalis
152.6
Category
152.6.1
152.7
View
152.7.1
Anterior View
153
RECTUS CAPITIS ANTERIOR
153.1
Origin
153.1.1 Anterior
surface of the lateral mass of the atlas and the root of its transverse process
153.2
Insertion
153.2.1 The
inferior surface of the basilar part of the occipital bone anterior to the
occipital condyle
153.3
Action
153.3.1 Aids
in flexion of the head at the neck
153.4
Nerve Supply
153.4.1 Ventral
rami of C1, 2
153.5
Synergists
153.5.1 Sternocleidomastoid,
longus calli, longus capitis
153.6
Category
153.6.1
153.7
View
153.7.1
Anterlor
View
154
RECTUS CAPITIS LATERALIS
154.1
Origin
154.1.1 Superior
surface of the transverse processes of the atlas
154.2
Insertion
154.2.1 Inferior
surface of the jugular process of the occipital bone
154.3
Action
154.3.1 Aids
in lateral flexion of the head on the neck
154.4
Nerve Supply
154.4.1 Ventral
rami of C1, 2
154.5
Synergists
154.5.1 :
Longus capitis, longissimus capitis, semispinalis capitis
154.6
Category
154.7
View
154.7.1
Anterior View
155
RECTUS CAPITIS POSTERIOR MAJOR
155.1
Origin
155.1.1 From
the spinous process of the axis
155.2
Insertion
155.2.1 The
lateral part of the inferior nuchal line of the occipital bone and the surface
of the bone immediately inferior to the line
155.3
Action
155.3.1 Extends
the head and rotates it to the same side
155.4
Nerve Supply
155.4.1 Suboccipital
nerve, dorsal ramus of C1
155.5
Synergists
155.5.1 Rectus
capitis posterior minor, obliquus capitis superior, longissimus capitis,
semispinalis capitis
155.6
Category
155.6.1
155.7
View
155.7.1
Posterior View
156
RECTUS CAPITIS POSTERIOR MINOR
156.1
Origin
156.1.1 The
tubercle on the posterior arch of the atlas
156.2
Insertion
156.2.1 The
medial part of the inferior nuchal line of the occipital bone and the surface
between it and the foramen mag- num
156.3
Action
156.3.1 Extends
the head at the neck
156.4
Nerve Supply
156.4.1 Suboccipital
nerve, dorsal ramus C1
156.5
Synergists
156.5.1 Rectus
capitis posterior major, obliquus capitis superior, longissimus capitis,
semispinalis capitis
156.6
Category
156.6.1
156.7
View
156.7.1
Posterior View
157
RECTUS FEMORIS (Quadriceps Femoris)
(1 of 4 Quadriceps)
157.1
Origin
157.1.1 STRAIGHT
HEAD
157.1.1.1
Anterior inferior iliac spine
157.1.2 REFLECTED
HEAD
157.1.2.1
Groove on upper brim of acetabulum
157.2
Insertion
157.2.1 Upper
border of patella and through the patellar ligament into tibial tuberosity
157.3
Action
157.3.1 Extension
of leg at the knee
157.3.2 Flexion
of thigh at the hip
157.3.3 REVERSED
ORIGIN-INSERTION ACTION
157.3.3.1 Flexes
the pelvis on the femur and gives anterior stabilization to the pelvis
157.4
Nerve Supply
157.4.1 Femoral,
L2, 3, 4
157.5
Synergists
157.5.1 Psoas,
sartorius, tensor fasciae latae, vasti lateralis, medialis and intermedius
157.6
Category
157.6.1
157.7
View
157.7.1
Anterior View
158
RHOMBOID MAJOR
158.1
Origin
158.1.1 Spinous
processes of 2nd -5th thoracic vertebrae
158.2
Insertion
158.2.1 Medial
border of scapula from spine to inferior angle
158.3
Action
158.3.1 Retracts
and elevates the scapula
158.3.2 The
inferior fibers aid in rotating the glenoid cavity inferiorly
158.4
Nerve Supply
158.4.1 Dorsal
scapular, C4, 5
158.5
Synergists
158.5.1 Upper,
middle and lower trapezius, levator scapulae, latissimus dorsi, rhomboid minor
158.6
Category
158.6.1
158.7
View
158.7.1
Posterior View
159
RHOMBOID MINOR
159.1
Origin
159.1.1 Lower
part of ligamentum nuchae, spinous processes of C7 and T1
159.2
Insertion
159.2.1 Medial
border of scapula at the root of the spine of the scapula
159.3
Action
159.3.1 Retracts
and elevates the scapula. Assists in rotating the scapula downwards
159.4
Nerve Supply
159.4.1 Dorsal
scapular, C4, 5
159.5
Synergists
159.5.1 Upper,
middle and lower trapezius, levator scapulae, latissimus dorsi and rhomboid
major
159.6
Category
159.6.1
159.7
View
159.7.1
Posterior View
160
RISORIUS
160.1
Origin
160.1.1 Parotid
fascia over the masseter muscle
160.1.2 (Note:
There are numerous variations)
160.2
Insertion
160.2.1 The
angle of the mouth
160.3
Action
160.3.1 Retracts
the angle of mouth
160.4
Nerve Supply
160.4.1 Inferior
buccal branch of the facial nerve (VII)
160.5
Arterial Supply
160.5.1 Branches
from the facial and transverse facial arteries
160.6
Synergists
160.6.1 Zygomaticus
major and buccinator
160.7
Antagonist
160.7.1 Orbicularis
oris
160.8
Category
160.8.1
161
ROTATORES BREVIS
161.1
Origin
161.1.1 A
series of pairs of small muscles extending from the sacrum to the axis
161.1.2 Transverse
processes of the vertebrae
161.2
Insertion
161.2.1 Bases
of the spinous processes (lamina) of the 1st vertebra above
161.3
Action
161.3.1 Acting
unilaterally, rotation of the spine to the opposite side. Acting bilaterally,
extension of the spine
161.4
Nerve Supply
161.4.1 Dorsal
rami of the spinal nerves
161.5
Synergists
161.5.1 Intertransversarii,
interspinales, multifidus and rotatores longus
161.6
Category
161.6.1
161.7
161.7.1
Posterior View
162
ROTATORES LONGUS
162.1
Origin
162.1.1 A
series of pairs of small muscles extending from the sacrum to the axis
162.1.2 Transverse
processes of the vertebrae
162.2
Insertion
162.2.1 Bases
of the spinous processes (lamina) of the 2nd vertebra above
162.3
Action
162.3.1 Acting
unilaterally, rotation of the spine to the opposite side. Acting bilaterally,
extension of the spine
162.4
Nerve Supply
162.4.1 Dorsal
rami of the spinal nerves
162.5
Synergists
162.5.1 Intertransversarii,
interspinales, multifidus and rotatores brevis
162.6
Category
162.6.1
162.7
View
162.7.1
Posterior View
163
SALPINGOPHARYNGEUS
163.1
Origin
163.1.1 Inferior part of the cartilaF.e of the auditory
tube (torus tubarius) near the tube's phafYngearopening
163.2
Insertion
163.2.1 Blends with palatopharyngeus
163.3
Action
163.3.1 Elevation of the upper lateral
pharyngeal wall
163.4
Nerve Supply
163.4.1 Pharyngeal branch of the va~s (X), with
the skeletomotor
branches from the cranial parts of tb:e spinal accessory nerve that pass
through the pliaryngeal plexus
163.5
Arterial
Supply
163.5.1 Greater palatine branch of the
maxillary artery; the ascending palatine and tonsillar branches of the facial
artery; a variable ramus from the ascending pharyngeal artery
163.6
Synergists
163.6.1 Palatopharyngeus and stylopharyngeus
163.7
Antagonists
163.7.1 Infrahyoid muscles lower pharynx during
late stages of swalloWIng
163.8
Category
163.8.1
163.9
View
163.9.1
The palatopharyngeus muscle has also been
illustrated
164
SARTORIUS
164.1
Origin
164.1.1 Anterior
superior iliac spine and upper half of the notch below it
164.2
Insertion
164.2.1 Anterior
and medial surface of the shaft of the tibia just below the condyle
164.3
Action
164.3.1 Flexes,
laterally rotates and abducts the thigh. Flexes and assists in medial rotation
of the leg
164.3.2 Reversed
origin-insertion action
164.3.2.1 When
femur and knee are fixed, flexes the pelvis on the hip and gives anterior
stabilization to the pelvis
164.4
Nerve Supply
164.4.1 Femoral,
L2, 3
164.5
Synergists
164.5.1 Biceps
femoris, semitendinous, semi- membranosus, gracilis
164.6
Category
164.6.1
164.7
VIew
164.7.1
Anterior View
165
SCALENUS ANTERIOR
165.1
Origin
165.1.1 Scalene
tubercle and ridgeon superior surface of the 1 st rib
165.2
Insertion
165.2.1 Anterior
tubercles of the transverse processes of the 3rd -6th cervicle vertebrae
165.3
Action
165.3.1 Acting
unilaterally, flexes and rotates cervical spine to the opposite side. When
acting bilaterally, flexes the neck and raises the 1st rib
165.4
Nerve Supply
165.4.1 Ventral
rami, C4,5,6
165.5
Synergists
165.5.1 Sternocleidomastoid,
scalenus medius and scalenus posterior, longus capitis, longus colli,
suprahyoid, infrahyoid and the platysma
165.6
Category
165.6.1
165.7
View
165.7.1
Anterior View
166
SCALENUS MEDIUS
166.1
Origin
166.1.1 Superior
surface of the 1 st rib behind subclavian groove
166.2
Insertion
166.2.1 Posterior
tubercles of the transverse processes of 2nd -7th cervical vertebrae
166.3
Action
166.3.1 Acting
unilaterally, laterally flexes and rotates cervical spine to the opposite side.
When acting bilaterally, flexes the neck and raises the 1 sI rib
166.4
Nerve Supply
166.4.1 Ventral
rami of C3 -8
166.5
Synergists
166.5.1 Sternocleidomastoid,
scalenus anterior and scalenus posterior, longus capitis, longus colli,
suprahyoid, infrahyoid and the platysma
166.6
Category
166.6.1
166.7
VIew
166.7.1
Anterior View
167
SCALENUS POSTERIOR
167.1
Origin
167.1.1 Outer
surface of 2nd rib behind attachment of serratus anterior
167.2
Insertion
167.2.1 Posterior
tubercles of transverse processes of 4th, 5th and 6th cervical vertebrae
167.3
Action
167.3.1 Acting
unilaterally, laterally flexes and rotates cervical spine to the opposite side.
When acting bilaterally, flexes the neck and raises the 2nd rib
167.4
Nerve Supply
167.4.1 Ventral
rami, C6,7,8
167.5
Synergists
167.5.1 Scalenus
medius, scalenus anterior, sternocleidomastoid, longus capitis, longus colli,
suprahyoid, infrahyoid and the platysma
167.6
Category
167.6.1
167.7
VIew
167.7.1
Anterior View
168
SEMIMEMBRANOSUS (Medial
Hamstring)
168.1
Origin
168.1.1 Upper
and lateral aspect of ischial tuberosity
168.2
Insertion
168.2.1 Posterior
surface of medial condyle of the tibia
168.3
Action
168.3.1 Flexes
and medially rotates the leg at the knee. Extends, adducts and medially rotates
the thigh at the hip
168.3.2 Reversed
origin-insertion action
168.3.2.1 When
the thigh is fixed, gives posterior stability to the pelvis and extends the
pelvis on the hip
168.4
Nerve Supply
168.4.1 Sciatic
(tibial portion), L5, S1, 2
168.5
Synergists
168.5.1 Semitendinosus,
biceps femoris, gastrocnemius, gracilis, sartorius
168.6
Category
168.6.1
168.7
View
168.7.1
Posterior View
169
SEMISPINALIS CAPITIS
169.1
Origin
169.1.1 7th
cervical and 1st -6th thoracic transverse processes and articular processes of
4th, Sth and 6th cervical vertebrae
169.2
Insertion
169.2.1 Between
superior and inferior nuchal lines of the occipital bone
169.3
Action
169.3.1 Extension
and lateral flexion of the neck and head, and rotation to the opposite side
169.4
Nerve Supply
169.4.1 Dorsal
rami of the cervical nerves
169.5
Synergists
169.5.1 Splenius
group, semispinalis cervicis
169.6
Category
169.6.1
169.7
View
169.7.1
Posterior View
170
SEMISPINALIS CERVICIS
170.1
Origin
170.1.1 Transverse
processes of the 1st -6th thoracic vertebrae
170.2
Insertion
170.2.1 Spinous
processes of 2nd -5th cervical vertebrae
170.3
Action
170.3.1 Acting
bilaterally, extension of the cervical spine
170.3.2 Acting
unilaterally, lateral flexion of the neck and head and rotation ot the opposite
side
170.4
Nerve Supply
170.4.1 Dorsal
rami of the cervical nerves
170.5
Synergists
170.5.1 Semispinalis
capitis, splenius cervicis, iliocostalis cervicis, longissimus capitis,
longissimus cervicis
170.6
Category
170.6.1
170.7
View
170.7.1
Posterior View
171
SEMISPINALIS THORACIS
171.1
Origin
171.1.1 The
transverse processes of the 6th -1Oth thoracic ver- tebrae
171.2
Insertion
171.2.1 The
spinous processes of the 1st -4th thoracic and the 6th and 7th cervical
vertebrae
171.3
Action
171.3.1 Extends
the spine and rotates it towards the opposite side
171.4
Nerve Supply
171.4.1 Dorsal
rami of the thoracic nerves, T1 -6
171.5
Synergists
171.5.1 Longissimus
thoracis, iliocostalis thoracis, spinalis thoracis
171.6
Category
171.6.1
171.7
View
171.7.1
Posterior View
172
SEMITENDINOSUS (Medial
Hamstring)
172.1
Origin
172.1.1 :
Ischial tuberosity with tendon of the long head of the biceps femoris
172.2
Insertion
172.2.1 Anterior
and medial surface of the shaft of the tibia just below the condyle
172.3
Action
172.3.1 Flexes
and medially rotates the leg at the knee. Extends, adducts and medially rotates
the thigh at the hip
172.3.2 Reversed
origin-insertion action
172.3.2.1 When
thigh is fixed, assists posterior stability of the pelvis and extends the
pelvis on the hip
172.4
Nerve Supply
172.4.1 Sciatic
(tibial portion), L5, 51, 2
172.5
Synergists
172.5.1 Semimembranosus,
biceps femoris, gastroc- nemius, gracilis, sartorius
172.6
Category
172.6.1
172.7
View
172.7.1
Posterior View
173
SERRATUS ANTERIOR
173.1
Origin
173.1.1 Superior
lateral surfaces of upper 8 or 9 ribs at the side of the chest
173.2
Insertion
173.2.1 Costal
surface of the vertebral border along the inferior angle of scapula
173.3
Action
173.3.1 Protracts
scapula and rotates it upwards to point the glenoid cavity superiorly.
Stabilizes vertebral border of scapula to thoracic cage, along with rhomboids
and middle trapezius
173.4
Nerve Supply
173.4.1 Long
thoracic, C5, 6, 7. SYNERGIST: Pectoralis minor
173.5
Synergists
173.5.1
173.6
Category
173.7
View
173.7.1
Lateral View
173.7.2
The scapula is pulled back off the rib cage to
view the anterior surface of the scapula
174
SERRATUS POSTERIOR INFERIOR
174.1
Origin
174.1.1 Spinous
processes of 11 th and 12th thoracic and 1 st, 2nd and 3rd lumbar vertebrae,
and the thoracolumbar fascia
174.2
Insertion
174.2.1 Inferior
borders of lower 4 ribs just beyond their angles
174.3
Action
174.3.1 Counteracts
the pull of the diaphragm by drawing the ribs posterior and inferior, aids in
respiration
174.4
Nerve Supply
174.4.1 Ventral
rami of T9 -12. SYNERGISTS: Internal intercostals
174.5
Synergists
174.5.1
174.6
Category
174.6.1
174.7
View
174.7.1
Posterior View
175
SERRATUS POSTERIOR SUPERIOR
175.1
Origin
175.1.1 Lower
portion of ligamentum nuchae and spinous processes of the 7th cervical and 1st,
2nd and 3rd thoracic ver- tebrae
175.2
Insertion
175.2.1 Superior
borders of 2nd -5th ribs distal to the angles
175.3
Action
175.3.1 Elevates
the ribs and is a muscle of inspiration
175.4
Nerve Supply
175.4.1 Ventral
rami of T2 -5
175.5
Synergists
175.5.1 Levatores
costarum breves, scalenus posterior
175.6
Category
175.6.1
175.7
View
175.7.1
Posterior View
176
SOLEUS
Back
Table of Contents References
176.1
Attachments
176.1.1 Origin
176.1.1.1 Posterior
surface of the head and upper 1/3 of the shaft of the fibula
176.1.1.2 Soleal
line and middle 1/3 of the medial border of the tibia
176.1.1.3 Tendinous
arch between tibia and fibula
176.1.2 Insertion
176.1.2.1 Into
calcaneus with gastrocnemius by way of the Achilles tendon
176.2
Action
176.2.1 Plantar
flexion and inversion of the foot at the ankle
176.2.2 Reversed
origin-insertion action
176.2.2.1 When
standing, the calcaneus becomes the fixed origin of the muscle. The soleus
muscle stabilizes the tibia on the calcaneus limiting forward sway
176.2.3
176.3
Nerve Supply
176.3.1 Nerve
176.3.1.1 Tibial
176.3.2 Roots
176.3.2.1 L5
176.3.2.2
S1
176.3.2.3 S2
176.4
Synergists
176.4.1 Gastrocnemius
176.4.2 Plantaris
176.4.3 Tibialis
Posterior
176.4.4 Peroneus
Longus and Brevis
176.4.5 Flexor
Hallucis Longus
176.4.6 Flexor
Digitorum Longus
176.5
Muscle Tests
176.5.1
176.6
Trigger Points
176.6.1 SOLEUS
176.7
Discussion (Gray)
176.7.1 The Soleus is a
broad flat muscle situated immediately in front of the Gastrocnemius. It arises
by tendinous fibers from the back of the head of the fibula, and from the upper
third of the posterior surface of the body of the bone; from the popliteal
line, and the middle third of the medial border of the tibia; some fibers also
arise from a tendinous arch placed between the tibial and fibular origins of the
muscle, in front of which the popliteal vessels and tibial nerve run. The
fibers end in an aponeurosis which covers the posterior surface of the muscle,
and, gradually becoming thicker and narrower, joins with the tendon of the
Gastrocnemius, and forms with it the tendo calcaneus. 15
176.7.2
176.7.3 Variations.—Accessory
head to its lower and inner part usually ending in the tendocalcaneus, or the
calcaneus, or the laciniate ligament.
16
176.7.4 The Gastrocnemius and Soleus together form a
muscular mass which is occasionally described as the Triceps suræ; its tendon
of insertion is the tendo calcaneus.
17
176.7.5
176.7.6 Tendo Calcaneus
(tendo Achillis).—The tendo calcaneus, the common tendon of the Gastrocnemius
and Soleus, is the thickest and strongest in the body. It is about 15 cm. long,
and begins near the middle of the leg, but receives fleshy fibers on its
anterior surface, almost to its lower end. Gradually becoming contracted below,
it is inserted into the middle part of the posterior surface of the calcaneus,
a bursa being interposed between the tendon and the upper part of this surface.
The tendon spreads out somewhat at its lower end, so that its narrowest part is
about 4 cm. above its insertion. It is covered by the fascia and the
integument, and is separated from the deep muscles and vessels by a
considerable interval filled up with areolar
176.7.7 Discussion
176.7.7.1 http://www.bartleby.com/107/129.html
176.7.8 Illustration
176.7.8.1 http://www.bartleby.com/107/illus438.html
176.7.8.2 http://www.bartleby.com/107/illus440.html
176.8
Category
176.8.1 Foot
& Toes (Posterior Superficial Compartment)
176.9
View
176.9.1
Posterior View
176.9.1.1 Posterior View (SOLEUS)
177
SPHINCTER PUPILLAE
177.1
Origin/Insertion
177.1.1 From collagenous connective tissue at
the pupillary end 0( the dilator muscle passing circumferentially around the
pupiL
177.2
Action
177.2.1 Constriction of the pupil to adjust to
near vision by increasing the depth of focus and/ or to increased light
177.3
Nerve Supply
177.3.1 Para~pathetic fibers through the
oculomotor nerve (III) from the Edmger-Westphal nucleus
177.4
Arterial
Supply
177.4.1 Long posterior and anterior ciliary
rami from the ophthalmic and lacrimal branches of the internal carotid artery
177.5
Synergists
177.5.1 None
177.6
Antagonist
177.6.1 Dilator pupillae
177.7
Category
177.7.1
177.8
View
177.8.1
The
lower s are enlarged horizontal sections
178
SPINALIS CAPITIS
178.1
Origin
178.1.1
178.2
Insertion
178.2.1
178.3
Action
178.3.1
178.4
Nerve Supply
178.4.1
178.5
Synergists
178.5.1
178.6
Category
178.6.1
179
SPINALIS CERVICIS
179.1
Origin
179.1.1 The
lower portion of the ligamentum nuchae, spinous processes of the 7th cervical and
sometimes the 1st and 2nd thoracic vertebrae
179.2
Insertion
179.2.1 The
spinous process of the axis and sometimes the 3rd and 4th cervical spinous
processes
179.3
Action
179.3.1 Acting
unilaterally, lateral flexion of the spine. Acting bilaterally, extension of
the spine
179.4
Nerve Supply
179.4.1 Dorsal
rami of the spinal nerves
179.5
Synergists
179.5.1 Longissimus
cervicis, semispinalis cervicis, splenius cervicis, iliocostalis cervicis
179.6
Category
179.6.1
179.7
View
179.7.1
Posterior View
180
SPINALIS THORACIS
180.1
Origin
180.1.1 The
spinous processes of the 1st and 2nd lumbar ver- tebrae, the thoracic vertebrae
11 and 12
180.2
Insertion
180.2.1 The
spinous processes of the upper thoracic ver- tebrae varying from 4 -8
180.3
Action
180.3.1 Acting
unilaterally, lateral flexion of the spine. Acting bilaterally, extension of
the spine
180.4
Nerve Supply
180.4.1 Dorsal
rami of the spinal nerves
180.5
Synergists
180.5.1 Semispinalis
thoracis, longissimus thoracis, iliocostalis thoracis, iliocostalis lumborum,
longissimus thoracis, quadratus lumborum
180.6
Category
180.6.1
180.7
VIew
180.7.1
Posterior View
181
SPINCTER ANI EXTERNUS
181.1
Origin
181.1.1
181.2
Insertion
181.2.1
181.3
Action
181.3.1
181.4
Nerve Supply
181.4.1
181.5
Synergists
181.5.1
181.6
Category
181.6.1
182
SPLENIUS CAPITIS
182.1
Origin
182.1.1 Spinous
processes of C7- T3, inferior half of ligamentum nuchae
182.2
Insertion
182.2.1 Mastoid
process and lateral third of the superior nuchal line
182.3
Action
182.3.1 Acting
bilaterally, extends the head and neck. Acting unilaterally, laterally flexes and
rotates head and neck to the same side
182.4
Nerve Supply
182.4.1 Dorsal
rami of the middle cervical spinal nerves
182.5
Synergists
182.5.1 Splenius
cervicis, semispinalis capitis, semi- spinalis cervicis, superior portion of
the trapezius
182.6
Category
182.6.1
Posterior View
183
SPLENIUS CERVICIS
183.1
Origin
183.1.1 Spinous
processes of 3rd -6th thoracic vertebrae
183.2
Insertion
183.2.1 1st,
2nd, 3rd and sometimes the 4th cervical ver- tebrae transverse processes on the
posterior aspect
183.3
Action
183.3.1 Acting
bilaterally, extends the head and neck. Acting unilaterally, laterally flexes
and rotates the neck to the same side
183.4
Nerve Supply
183.4.1 Dorsal
rami of the lower cervical spinal nerves
183.5
Synergists
183.5.1 Splenius
capitis, semispinalis capitis, semispinalis cervicis, superior portion of
trapezius, for extension and lateral flexion
183.6
Category
183.6.1
183.7
View
183.7.1
Posterior View
184
STAPEDIUS
184.1
Origin
184.1.1 From
the. poster!or wall of the tympanic cavity, a conical caVIty In the pyramidal
emInence
184.2
Insertion
184.2.1 The
posterior surface on the neck of the stapes
184.3
Action
184.3.1 Pulls
the head of the stapes posteriorly, fiXing the ossicular c~ai.n (malleus. incus
and stapes) and, ~hereby, reducing the tranSm1SSlOn of sound energy through the
middle ear
184.4
Nerve Supply
184.4.1 Stapedial
branch of the facial nerve (VII)
184.5
Arterial Supply
184.5.1 Stylomastoid
branch of the occipital or posterior auricular artenes. Other arteries of the
tympanic cavity; superior tympanic branch of the middle meningeal arle!y, the
anlerior: tympanic branch of th~ maxillary artery, the inferior tymp~mc branc\t
of the ascend1f!g pharyngeal.artery and the carot1COtympamc branch of the
Internal carot1d artery
184.6
Synergists
184.6.1 The
te!lsor tympani and stapedius act together to tense the ossicular cham
184.7
Antagonist
184.7.1 None
184.8
Category
184.8.1
185
STERNALIS
185.1
Origin
185.1.1
185.2
Insertion
185.2.1
185.3
Action
185.3.1
185.4
Nerve Supply
185.4.1
185.5
Synergists
185.5.1
185.6
Category
185.6.1
186
STERNOCLEIDOMASTOID
186.1
Origin
186.1.1 Sternal
Head
186.1.1.1 Anterior
surface of the manubrium
186.1.2 Clavicular
Head
186.1.2.1 Superior
surface of the medial 1/3 of the clavicle
186.2
Insertion
186.2.1 Lateral
surface of the mastoid process of the tem- poral bone and lateral half of the
superior nuchal line of the occipital bone
186.3
Action
186.3.1 Acting
unilaterally, draws the head toward the ipsilateral shoulder and rotates the
head to the opposite side. Acting bilateral- ly, flexes the head
186.4
Nerve Supply
186.4.1 Ventral
rami of C2, 3. Spinal portion of the accessory nerve (cranial X1)
186.5
Synergists
186.5.1 Scalene
group
186.6
Category
186.6.1
186.7
View
186.7.1
Anterior View
187
STERNOHYOID (INFRAHYOID)
187.1
Origin
187.1.1 The posterior aspect of the clavicle
and the upper posterior aspect of the manubrium sterni
187.2
Insertion
187.2.1 Inferior border of the hyoid body
187.3
Action
187.3.1 Hyoid depression
187.4
Nerve Supply
187.4.1 Ansa cervicalis (Cl, C2, C3)
187.5
Arterial
Supply
187.5.1 Muscular branches from the superior and
inferior thyroid arteries
187.6
Synergists
187.6.1 Other infrahyoid muscles (thyrohyoid,
omohyoid and sternothyroid)
187.7
Antagonists
187.7.1 Supra~yoid muscles (e.g., stylohyoid,
digastric, gemohyold and mylollyolCl)
187.8
Category
187.8.1
188
STERNOTHYROID (INFRAHYOID)
188.1
Origin
188.1.1 The
posterior manubrial surface inferior to the ste~ohyoid orIgin, and to the
posterior edge of the fIrst costal cartIlage
188.2
Insertion
188.2.1 The
oblique line on the thyroid lamina
188.3
Action
188.3.1 Depression
of the elevated larynx
188.4
Nerve Supply
188.4.1 Ansa
cervicalis (Cl, C2, C3)
188.5
Arterial Supply
188.5.1 Muscular
branches from the superior and inferior thyroid arteries
188.6
Synergists
188.6.1 All
infrahyoid muscles lower the hyoid bone and, therefore, mdIrectly the larynx
188.7
Antagonists
188.7.1 Thyrohyoid
and, indirectly, the suprahyoid muscles
188.8
Category
188.8.1
189
STYLOGLOSSUS
189.1
Origin
189.1.1 Anterior and lateral aspect of the
styloid process, near its apex and from the styloid end of the stylomandibu1ar
ligament
189.2
Insertion
189.2.1 Lon~itudinal part
189.2.1.1 Blend with the inferior longitudinal
muscle in front of the hypoglossus
189.2.2 Oblique part
189.2.2.1 Overlapping and decussating with the
hyoglossus
189.3
Action
189.3.1 Draw the tongue up and backwards
189.4
Nerve Supply
189.4.1 Hypoglossal nerve (XII)
189.5
Arterial
Supply
189.5.1 Lingual arteries and its branches; dorsal
lingual and sublingual rami. Tonsitlar rami of the facial artery
189.6
Synergists
189.6.1 Palatoglossus
189.7
Antagonists
189.7.1 Hyoglossus and genioglossus
189.8
Category
189.8.1
189.9
View
189.9.1
The
styloid process and mastoid process have been superimposed to this sagittal
section
190
STYLOHYOID (SUPRAHYOID)
190.1
Origin
190.1.1 Posterior aspect of styloid process
near its base
190.2
Insertion
190.2.1 Splits around digastric muscle
(posterior belly) and is attached to hyoid body at its junction with the
greater cornu
190.3
Action
190.3.1 Elevates and retracts the hyoid bone
190.4
Nerve Supply
190.4.1 Stylohyoid branch of the facial nerve
(VII)
190.5
Arterial
Supply
190.5.1 Posterior auricular artery and muscular
branches of the occipital artery
190.6
Synergists
190.6.1 For. the. hyoid elevation
190.6.1.1 Digastric, mylohyoid and gemohyold
190.7
Antagonists
190.7.1 For the. hyoid elevation
190.7.1.1 Sternohyoid, thyrohyoid and omohyoid
190.7.2 For hyoid retraction
190.7.2.1 Geniohyoid
190.8
Category
190.8.1
191
STYLOPHARYNGEUS
191.1
Origin
191.1.1 Medial side of the base of the styloid
process
191.2
Insertion
191.2.1 Blends between superior and middle
pharyngeal constrictors within the lateral glosso-eRiglottic fold, and with the
palatopharyngeus to the posterior borCler of the thyroid cartilage
191.3
Action
191.3.1 Elevation and dilation of the pharynx during
early phase of swallowing
191.4
Nerve Supply
191.4.1 Muscular branch of the glossopharyngeal
nerve
191.5
Arterial
Supply
191.5.1 Ascending pharyngeal artery, ascending
Ralatine artery, tonsillar artery, dOrsa11ing1;lal branch of the lingual artery
and rami from tne superior thyroid artery
191.6
Synergists
191.6.1 For pharyngeal elevation
191.6.1.1 Salpingopharyngeus and palatopharyngeus
191.6.2 For pharyngeal dilation
191.6.2.1 None
191.7
Antagonists
191.7.1 The infrahyoid muscles lower pharynx
during late stages of.sw~llowing. The pharyngeal constrictors oppose pharyngeal
dilatlon
191.8
Category
191.8.1
191.9
View
191.9.1
The
palatopharyngeus and the superior .and middle pharyngeal constrlctor muscles
have also been illustrated
192
SUBCLAVIUS
192.1
Origin
192.1.1 1st
rib at the junction of the costal cartilage
192.2
Insertion
192.2.1 Groove
on the inferior surface of the clavicle, between the costoclavicular and conoid
ligaments
192.3
Action
192.3.1 Depresses
clavicle, pulls it inferiorly and anteriorly
192.4
Nerve Supply
192.4.1 Subclavian
branch of the brachial plexus, C5, 6
192.5
Synergists
192.5.1
192.6
Category
192.6.1
192.7
View
192.7.1
Anterior View
193
SUBSCAPULARIS
(Rotator Cuff Muscle)
193.1
Origin
193.1.1 Entire
anterior surface of the subscapular fossa
193.2
Insertion
193.2.1 Lesser
tubercle of humerus and capsule of shoulder joint
193.3
Action
193.3.1 Medial
rotation of the humerus atthe shoulder. Stabiliza- tion of the glenohumeral
joint
193.3.2 Reversed
origin- insertion action
193.3.2.1 When
the humerus is stabilized, abducts the inferior border of the scapula
193.4
Nerve Supply
193.4.1 Upper
and lower subscapular, C5, 6, 7
193.5
Synergists
193.5.1 Teres
major, pectoralis major, latissimus dorsi
193.6
Category
193.6.1
193.7
View
193.7.1
Anterior View
194
SUPERFICIAL TRANSVERSE PERINEUS (SUPERFICIALIS)
194.1
Origin
194.1.1
194.2
Insertion
194.2.1
194.3
Action
194.3.1
194.4
Nerve Supply
194.4.1
194.5
Synergists
194.5.1
194.6
Category
194.6.1
195
SUPERIOR LONGITUDINAL LINGUALIS
195.1
Origin
195.1.1 The submucous fibrous tissue near the
epiglottis and the median fibrous septum
195.2
Insertion
195.2.1 The lingual apex and margins of the
tongue
195.3
Action
195.3.1 Shortens the tongue and turns the apex
and sides upwards to make the dorsum concave
195.4
Nerve Supply
195.4.1 Hypoglossal (XII)
195.5
Arterial
Supply
195.5.1 Lingual artery and its branches; dorsal
-lingual and sublingual rami
195.5.2 Tonsillar rami of the facial artery
195.6
Synergists
195.6.1 For shortening the tongue
195.6.1.1 Inferior longitudinal
195.7
Antagonist
195.7.1 For raising the apex and side
195.7.1.1 Inferior longitudinal
195.8
Category
195.8.1
196
SUPERIOR OBLIQUE
196.1
Origin
196.1.1 Body of the lesser wing, of the
sphenoid sureromedial
to the optic canal and to the tendinous attachment o the superior rectus
196.2
Insertion
196.2.1 After traversing the trochlea, the
fibrocartilaginous loop, the round tendon is Qeflected to the sclera behind the
equat.or in its superol~teral posterior quadrant, between the superIOr and
latera1 recti
196.3
Action
196.3.1 Elevates the posterior aspect of the
eye, hence, rotates the visu.al axis (and pupil) do~ward.s (de:presslon) and
laterally (abduction). In the anteroposterIor axIS, It mtorts the eye
196.4
Nerve Supply
196.4.1 Trochlear nerve (IV)
196.5
Arterial
Supply
196.5.1 Muscular branch of the ophthalmic
artery from the internal carotid artery
196.6
Synergists
196.6.1 Vertical axis
196.6.1.1 Lateral rectus and inferior oblique
196.6.2 Transverse axis
196.6.2.1 Inferior rectus
196.6.3 Anteroposterior axis
196.6.3.1 Superior rectus
196.7
Antagonists
196.7.1 Vertical axis: Superior rectus, medial
rectus, and inferior rectus
196.7.2 Transverse axis: Inferior oblique and
superior rectus
196.7.3 Anteroposterior axis: Inferior oblique
and inferior rectus
196.8
Category
196.8.1
196.9
Note
196.9.1
All
six extraocular muscles are involved, and act in concert during an eye
movement; synergists and antagonists depend on 1..t~ fixation point of the eye prior
to movement
197
SUPERIOR PHARYNGEAL CONSTRICTOR
197.1
Origin/Insertion
197.1.1 Anterior attachment: Pterygopharyngeal
part of hamulus on medial pterygoid plate
197.1.2 Buccopharyngeal part: Pterygomandibular
raphe
197.1.3 l\:Iylopharyngeal part: Posterior end
of the mylohyoid lme on mandible
197.1.4 Glossopharyngeal part: A few fibres to
the side of the tongue
197.1.5 Posterior attachments: The posterior
median pharyngeauaphe and by an apon~urosis to the pharyngeal tubercle on the
basilar part of the occipital bone
197.2
Action
197.2.1 General sphincteric and peristallic
action during swalloWing
197.3
Nerve Supply
197.3.1 Pharyngeal branch of the vagus (X),
with the skeletomotor branches from the cranial parts of the spinal accessory
nerve that pass through the pharyngeal plexus
197.4
Arterial
Supply
197.4.1 Ascending pharyngeal artery ascending
Ralatine and tonsillar branches Of the facial artery. Branches of the maxillary artery; greater palatine,
pha~gear and the artery of the pterygOia canal. tne dorsallingualDrancli of the
lingual artery
197.5
Synergists
197.5.1 Inferior and middle pharyngeal
constrictors
197.6
Antagonist
197.6.1 Stylopharyngeus dilates the pharynx
197.7
Category
197.7.1
198
SUPERIOR RECTUS
198.1
Origin
198.1.1 Superolateral margin of the optic canal
on the common annular tendon
198.2
Insertion
198.2.1 Anterosuperior margin of the eye into
the sclera about 7.7 mm posterior to the margin of the cornea
198.3
Action
198.3.1 Elevates the anterior aspect of the
eye, hense rotates eye in the transverse axis upwards (elevation). In the vertical
axis, it aids in I!1edia~ ~o~ation (adduction) of the eye. In the
anteroposterIor ax1S it mtorts the eye
198.4
Nerve Supply
198.4.1 Branch from the superior division of
the oculomotor nerve (III)
198.5
Arterial
Supply
198.5.1 Muscular rami from the supraorbital
branch of the ophthalmic artery
198.6
Synergists
198.6.1 Vertical axis: Medial and inferior
rectus.
198.6.2 Transverse axis: Inferior oblique. .
198.6.3 Anteroposterior axis: Superior oblique
198.7
Antagonists
198.7.1 Vertical axis: Inferior and superior
oblique, lateral rectus.
198.7.2 Transverse ttxis: Inferior rectus and
superior oblique.
198.7.3 Anteroposterior axis: Inferior rectus
and inferior oblique
198.8
Category
198.8.1
198.9
Note
198.9.1
All
six extraocular muscles are involved, and act in concert during an eye
movement; synergists and antagonists depend on the fiXation point of the eye
prior to movement
199
SUPINATOR ?
199.1
Origin
199.1.1 Lateral
epicondyle of humerus, radial collateral ligament of elbow, annular ligament of
radius and the supinator crest of ulna
199.2
Insertion
199.2.1 An
oblique line on the lateral anterior surface of the upper 1/3 of radius
199.3
Action
199.3.1 Supinates
the forearm
199.4
Nerve Supply
199.4.1 Posterior
interosseous, (deep radial) , C5, 6
199.5
Synergists
199.5.1 Biceps
brachii
199.6
Category
199.6.1
199.7
View
199.7.1
Posterlor View
200
SUPRASPINATUS (Rotator
Cuff Muscle)
200.1
Origin
200.1.1 Medial
'2/3 of supraspinous fossa
200.2
Insertion
200.2.1 Superior
surface of greater tubercle of humerus and capsule of shoulder joint
200.3
Action
200.3.1 Abduction
of humerus at the shoulder joint. Stabilization of the glenohumeral joint
200.4
Nerve Supply
200.4.1 Suprascapular,
C4, 5, 6
200.5
Synergists
200.5.1 Deltoid
200.6
Category
200.6.1
200.7
View
200.7.1
Posterior View
201
TEMPORALIS
201.1
Origin
201.1.1 Arises from the temporal fossa, and
from the deep surface of the temporal fascia
201.2
Insertion
201.2.1 Passing between th,e zygomatic arch and
cr,anial wall to the medial surface, aRex" antenor border of the coronold
process and border of the mand1bular ramus
201.3
Action
201.3.1 Closes the. jaw by the anterior fibers.
Posterior .fibers retract from protruslOn and thereby fiX the temporomand1bular
joint. The muscle is also concerned in lateral grinding movements
201.4
Nerve Supply
201.4.1 DeeR tem poral branches from the anterior trunk
of the mandibular division o the trigeminal nerve (V3)
201.5
Arterial
Supply
201.5.1 Deep temporal branches of the maxillary
artery... !Diddle temporal, frontal and parietal branches of the supemc1al
temporal artery
201.6
Synergists
201.6.1 For closing the jaw: Masseter and
medial pterygoids.
201.6.2 For retraction: None
201.7
Antagonists
201.7.1 For closipg the jaw:
I,.atera,l-pter;ygoiqs and th,e digastric, mylohyold \!nd gernohyolo wlien
1nfrahyold muscles contract to fiX hyOld bone.
201.7.2 For retraction from protrusion: Lateral
pterygoid
201.8
Category
201.8.1
201.9
View
201.9.1
The
zygomatic arch has been removed
202
TENSOR FASCIAE LATAE
202.1
Origin
202.1.1 Anterior
part of outer lip of iliac crest, outer surface of anterior superior iliac
spine
202.2
Insertion
202.2.1 Iliotibial
band of fascia lata on the anterolateral aspect of thigh, about 1/3 of the way
down
202.3
Action
202.3.1 Thigh
flexion at the hip, abduction, and medial rotation. Stabilizes the knee
laterally. Tenses the iliotibial tract
202.4
Nerve Supply
202.4.1 Superior
gluteal, L4, 5, S1
202.5
Synergists
202.5.1 Gluteus
medius, gluteus minimus, and upper fibers of the gluteus maximus
202.6
Category
202.6.1
202.7
View
202.7.1
Anterior and Lateral View
203
TENSOR TYMPANI
203.1
Origin
203.1.1 The cartilaginous part of the
pharyn~otympanic tube and the adjoining part of the greater wing of tile
sphenoid
203.2
Insertion
203.2.1 Reflected around the process
cochleariformis to the handle of the malleus near its root
203.3
Action
203.3.1 Pulls the malleus medially thereby
tensin,g the tyn:Ipanic membrane and fixing the ossicular chain (malleus, mcus
and stapes)
203.4
Nerve Supply
203.4.1 Bra1:tch of the ne1Ve to the, med,ial
pterygoid a ramus from the mandIbular branch of the trlgemmar nerve (V3)
203.5
Arterial
Supply
203.5.1 Superior tympanic ramus from the middle
meningeal branch of the maxillary artery, Other arteries of the tympanic
cavitY; the anterior tym ranic
Dranch of the maxillary arte;ry, the styll?mastoi~ bra,nch o the ,occipital or
posterior . aurIcular arterIes, the mferlor tympanIc branch oflhe ascendmg
pharyngeal artery and the caroticotympanic branch of the internal carotid
artery
203.6
Synergists
203.6.1 The te!lsor tympani and stapedius act
together to tense the ossIcular cham
203.7
Antagonist
203.7.1 None
203.8
Category
203.8.1
204
TENSOR VELI PALATINI
204.1
Origin
204.1.1 The
scaphoid fossa of the pterygoid process, the lateral lamina of the cartilage
part of the auditory tube and the medial aspect of the sphenoldaf spine
204.2
Insertion
204.2.1 By
a tendon turning around the hamulus of the medial pterygoid p!ate to the
.palatine aponeuro~is and the osseous surfaces behmd the palatme crest on the
honzontal plate of the palatine bone
204.3
Action
204.3.1 Unilaterally:
The muscle pulls the soft palate to the same side.
204.3.2 Bilaterally:
It tightens the soft palate, closing off the nasopharynx and oropharynx
204.4
Nerve Supply
204.4.1 Mandibular
branch of trigeminal nerve (V3)
204.5
Arterial Supply
204.5.1 Greater
palatine branch of the maxillary artery, the ascending palatine artery and the
ascending pharyngeal artery
204.6
Synergists
204.6.1 Levator
veli palatini for closing the nasopharynx
204.7
Antagonist
204.7.1 None
204.8
Category
204.8.1
205
TERES MAJOR
205.1
Origin
205.1.1 Dorsal
surface of inferior angle of the scapula on lower 1/3 of scapular axillary
border
205.2
Insertion
205.2.1 Medial
lip of intertubercular sulcus of humerus. Medial to latissimus dorsi tendon
205.3
Action
205.3.1 Adducts
and medially rotates humerus at the shoulder. Extends the shoulder joint.
REVERSED ORIGIN-INSERTION ACTION: When arm is fixed, adducts and elevates
inferior angle of scapula
205.4
Nerve Supply
205.4.1 Lower
subscapular, C6, 7
205.5
Synergists
205.5.1 Latissimus
dorsi, subscapularis
205.6
Category
205.6.1
205.7
View
205.7.1
Posterior View
206
TERES MINOR (Rotator
Cuff Muscle)
206.1
Origin
206.1.1 Superior
;?/3 of dorsal surface of axillary border of scapula:
206.2
Insertion
206.2.1 Inferior
aspect of greater tubercle of the humerus, capsule
of the shoulder joint
206.3
Action
206.3.1 Lateral
rotation of humerus at the shoulder, Stabilization of head of humerus. REVERSED
ORIGIN- INSERTION ACTION: When humerus is stabilized, abducts the inferior angle
of the scapula
206.4
Nerve Supply
206.4.1 Axillary,
C4, 5, 6
206.5
Synergists
206.5.1 Infraspinatus,
subscapularis
206.6
Category
206.6.1
206.7
View
206.7.1
Posterlor View
207
THYROARYTENOID VOCALIS & THYROEPIGLOTTICUS
207.1
Origin
207.1.1 The thyroid cartilage and cricothyroid
ligament
207.2
Insertion
207.2.1 Vocalis: To the vocal process and
anterolateral surface of the arytenoid cartilage. Thyroarytenoid: To the anterolateral
arytenoid suiface and upper fovea on it. Thyroepiglotticus: To the epiglottic
fold and margin
207.3
Action
207.3.1 Thyroarytenoid and vocalis: Draws the
arytenoid cartilages ventrally producing vocal fold relaxation. Th):roel?iglotticus: Abduction of the
aryepiglottic folCIs, widening the laryngeal inlet
207.4
Nerve Supply
207.4.1 Recurrent laryngeal branch of the vagus
(X)
207.5
Arterial
Supply
207.5.1 Laryngeal branches from the superior
and inferior thyroid arteries
207.6
Synergists
207.6.1 None
207.7
Antagonists
207.7.1 For vo.cal fqld tension. regulation:
Cricothyroids and posterIor CrICoarytenolds. For laryngeal ~nlet modification:
Oblique arytenoids ahJ aryeplglottlCUS
207.8
Category
207.8.1
208
THYTROHYOID (INFRAHYOID)
208.1
Origin
208.1.1 Oblique line of thyroid lamina
208.2
Insertion
208.2.1 Lower border of the greater cornu and
adjacent body of hyoid
208.3
Action
208.3.1 Hyoid depression and/or elevation of
the larynx
208.4
Nerve Supply
208.4.1 Branches of Cl traveling with the
hypoglossal nerve
208.5
Arterial
Supply
208.5.1 Superior thyroid artery and its
branches; infrahyoid~ cricohy<?id apd superior laryngeal arteries. Muscular
branches Ifom the mfenor thyroId artery
208.6
Synergists
208.6.1 For hyoid d~pression: Sternohyoid,
omohyoid and sternothyroId. For laryngeal elevation: Indirectly suprahyoid
muscles and stylopharyngeus
208.7
Antagonists
208.7.1 For .hyoid; depression: Digastric,
mylohyoid and gemohyold. For
laryngeal elevation: Sternothyroid
208.8
Category
208.8.1
209
TIBIALIS ANTERIOR
Back Table of Contents References
209.1
Attachments
209.1.1 Origin
209.1.1.1 Lateral
condyle of tibia
209.1.1.2 Proximal
2/3 of lateral surface of tibia
209.1.1.3 Interosseous
membrane
209.1.1.4 Deep
fascia
209.1.1.5 Lateral
intermuscular septum
209.1.2 Insertion
209.1.2.1 Plantar
surface of base of first metatarsal
209.1.2.2 Medial
plantar surface of first cuneiform
209.2
Action
209.2.1 Dorsiflexion
(Foot at ankle)
209.2.2 Inversion
(Foot at ankle)
209.2.3 REVERSED
ORIGIN-INSERTION ACTION
209.2.3.1 When
standing, the foot is fixed and becomes the origin
209.2.3.2 Action
causes forward body lean antagonistic to the plantar flexion of the soleus and
gastrocnemius.
209.2.3.3 Active
in the balance mechanism of anterior and posterior sway
209.3
Nerve Supply
209.3.1 Nerve
209.3.1.1 Deep
peroneal
209.3.2
Roots
209.3.2.1 L4
209.3.2.2 L5
209.3.2.3 S1
209.4
Synergists
209.4.1 Extensor
hallucis longus
209.4.2 Extensor
digitorum longus
209.5
Muscle Tests
209.5.1
209.6
Trigger Points
209.6.1
209.7
Discussion (Gray)
209.7.1 The Tibialis anterior
(Tibialis anticus) is situated on the lateral side of the tibia; it is thick
and fleshy above, tendinous below. It arises from the lateral condyle and upper
half or two-thirds of the lateral surface of the body of the tibia; from the
adjoining part of the interosseous membrane; from the deep surface of the
fascia; and from the intermuscular septum between it and the Extensor digitorum
longus. The fibers run vertically downward, and end in a tendon, which is
apparent on the anterior surface of the muscle at the lower third of the leg.
After passing through the most medial compartments of the transverse and
cruciate crural ligaments, it is inserted into the medial and under surface of
the first cuneiform bone, and the base of the first metatarsal bone. This
muscle overlaps the anterior tibial vessels and deep peroneal nerve in the
upper part of the leg. 3
209.7.2
209.7.3 Variations.—A deep
portion of the muscle is rarely inserted into the talus, or a tendinous slip
may pass to the head of the first metatarsal bone or the base of the first
phalanx of the great toe. The Tibiofascialis anterior, a small muscle from the
lower part of the tibia to the transverse or cruciate crural ligaments or deep
fascia.
209.7.4 Discussion
209.7.4.1 http://www.bartleby.com/107/129.html
209.7.5 Illustration
209.7.5.1 http://www.bartleby.com/107/illus437.html
209.7.5.2 http://www.bartleby.com/107/illus440.html
209.8
Category
209.8.1 Foot & Toes (Anterior
Compartment)
209.9
View
209.9.1
Anterior and Plantar View
210
TIBIALIS POSTERIOR
Back
Table of Contents References
210.1
Attachments
210.1.1 Origin
210.1.1.1 Lateral
part of posterior surface of tibia
210.1.1.2 Proximal
2/3 of medial surface of fibula
210.1.1.3 Interosseous
Membrane
210.1.1.4 Intermuscular
Septa
210.1.1.5 Deep
Fascia
210.1.2 Insertion
210.1.2.1 Tuberosity
of Navicular Bone
210.1.2.2 Sustenaculum
tali of calcaneus
210.1.2.3 Plantar
surfaces of all three cuneiforms
210.1.2.4 Cuboid
Bone
210.1.2.5 Bases
of the 2nd, 3rd and 4th metatarsal bones
210.2
Action
210.2.1 Inverts
and plantar flexes the foot at the ankle
210.2.2 Medial
ankle stabilizer
210.3
Nerve Supply
210.3.1 Nerve
210.3.1.1 Tibial
210.3.2 Roots
210.3.2.1 L4
210.3.2.2 L5
210.4
Synergists
210.4.1 Flexor
Hallucis Longus
210.4.2 Flexor
Digitorum Longus
210.5
Muscle Tests
210.5.1
210.6
Trigger Points
210.6.1 TIBIALIS
POSTERIOR
210.7
Discussion (Gray)
210.7.1 The Tibialis
posterior (Tibialis posticus) lies between the two preceding muscles, and is
the most deeply seated of the muscles on the back of the leg. It begins above
by two pointed processes, separated by an angular interval through which the
anterior tibial vessels pass forward to the front of the leg. It arises from
the whole of the posterior surface of the interosseous membrane, excepting its
lowest part; from the lateral portion of the posterior surface of the body of
the tibia, between the commencement of the popliteal line above and the
junction of the middle and lower thirds of the body below; and from the upper
two-thirds of the medial surface of the fibula; some fibers also arise from the
deep transverse fascia, and from the intermuscular septa separating it from the
adjacent muscles. In the lower fourth of the leg its tendon passes in front of
that of the Flexor digitorum longus and lies with it in a groove behind the
medial malleolus, but enclosed in a separate sheath; it next passes under the
laciniate and over the deltoid ligament into the foot, and then beneath the
plantar calcaneonavicular ligament. The tendon contains a sesamoid
fibrocartilage, as it runs under the plantar calcaneonavicular ligament. It is
inserted into the tuberosity of the navicular bone, and gives off fibrous
expansions, one of which passes backward to the sustentaculum tali of the
calcaneus, others forward and lateralward to the three cuneiforms, the cuboid,
and the bases of the second, third, and fourth metatarsal bones. 29
210.7.2 Nerves.—The
Popliteus is supplied by the fourth and fifth lumbar and first sacral nerves,
the Flexor digitorum longus and Tibialis posterior by the fifth lumbar and
first sacral, and the Flexor hallucis longus by the fifth lumbar and the first
and second sacral nerves, through the tibial nerve. 30
210.7.3 Actions.—The
Popliteus assists in flexing the leg upon the thigh; when the leg is flexed, it
will rotate the tibia inward. It is especially called into action at the
beginning of the act of bending the knee, inasmuch as it produces the slight
inward rotation of the tibia which is essential in the early stage of this
movement. The Tibialis posterior is a direct extensor of the foot at the
ankle-joint; acting in conjunction with the Tibialis anterior, it turns the
sole of the foot upward and medialward, i.e., inverts the foot, antagonizing
the Peronæi, which turn it upward and lateralward (evert it). In the sole of
the foot the tendon of the Tibialis posterior lies directly below the plantar
calcaneonavicular ligament, and is therefore an important factor in maintaining
the arch of the foot. The Flexor digitorum longus and Flexor hallucis longus
are the direct flexors of the phalanges, and, continuing their action, extend
the foot upon the leg; they assist the Gastrocnemius and Soleus in extending
the foot, as in the act of walking, or in standing on tiptoe. In consequence of
the oblique direction of its tendons the Flexor digitorum longus would draw the
toes medialward, were it not for the Quadratus plantæ, which is inserted into
the lateral side of the tendon, and draws it to the middle line of the foot.
Taking their fixed point from the foot, these muscles serve to maintain the
upright posture by steadying the tibia and fibula perpendicularly upon the
talus.
210.7.4 Discussion
210.7.4.1 http://www.bartleby.com/107/129.html
210.7.5 Illustration
210.7.5.1 http://www.bartleby.com/107/illus439.html
210.7.5.2 http://www.bartleby.com/107/illus440.html
210.8
Category
210.8.1 Foot
& Toes (Posterior Deep Compartment)
210.9
VIew
210.9.1
Posterior and Plantar View
210.9.1.1 Posterior and Plantar View (TIBIALIS POSTERIOR)
211
TRANSVERSUS ABDOMINIS
211.1
Origin
211.1.1 :
Lateral 1/3 of the inquinalligament, anterior ';/3 of inner lip of the iliac
crest, thoracolumbar fascia and from the inner edges of the lower 6 costal
cartilages
211.2
Insertion
211.2.1 The
linea alba by its aponeurosis
211.3
Action
211.3.1 Constricts
abdominal contents; assists in forced expira- tion
211.4
Nerve Supply
211.4.1 Branches
of the 7th .12th intercostal and the iliohypogastric and ilioinquinal nerves, L
1
211.5
Synergists
211.5.1
211.6
Category
211.6.1
211.7
View
211.7.1
Lateral View
212
TRANSVERSE ARYTENOID
212.1
Origin/Insertion
212.1.1 Arises from, and inserts onto, the
medial aspects of the contralateral muscular process and posterior suifaces of
arytenoids
212.2
Action
212.2.1 The a~enoid cartilages are adducted and
the attached vocal folds close (closure of the rima glottis)
212.3
Nerve Supply
212.3.1 Recurrent laryngeal branch of the vagus
nerve (X)
212.4
Arterial
Supply
212.4.1 SuRerior laryngeal branch of the
suRerior thyroid artery and the inferior laryngeal branch of the inferior
thyroid artery
212.5
Synergists
212.5.1 Lateral cricoarytenoids
212.6
Antagonist
212.6.1 Posterior cricoarytenoids
212.7
Category
212.7.1
213
TRANSVERSE LINGUALIS (BODY OF TONGUE)
213.1
Origin
213.1.1 Median fibrous septum
213.2
Insertion
213.2.1 The submucous fibrous tissue at the lingual
margin, posteriorly blending with the palatoglossal muscle (via palatoglossal
arch)
213.3
Action
213.3.1 Narrows and elongates the tongue
213.4
Nerve Supply
213.4.1 Hypoglossal nerve (XII)
213.5
Arterial
Supply
213.5.1 Lingual artery and its branches, dorsal
lingual and sublingual rami. Tonsillar rami of the facial artery
213.6
Synergists
213.6.1 None
213.7
Antagonist
213.7.1 None
213.8
Category
213.8.1
214
TRANSVERSE PERINEUS (PROFUNDUS)
214.1
Origin
214.1.1
214.2
Insertion
214.2.1
214.3
Action
214.3.1
214.4
Nerve Supply
214.4.1
214.5
Synergists
214.5.1
214.6
Category
214.6.1
215
TRAPEZIUS LOWER (Lower Division)
215.1
Origin
215.1.1 Spinous
processes of 6th -12th thoracic vertebrae
215.2
Insertion
215.2.1 Medial
1/3 of spine of the scapula
215.3
Action
215.3.1 Depresses
the scapula. Retracts the scapula. Rotates the scapula upwards so the glenoid
cavity faces superiorly. Gives inferior stabilization of scapula-,fJds to maintain
spine in extension
215.4
Nerve Supply
215.4.1 Spinal
accessory and ventral rami C3, 4
215.5
Synergists
215.5.1 Trapezius
upper and lower divisions
215.6
Category
215.6.1
215.7
View
215.7.1
Posterior
View
216
TRAPEZIUS MIDDLE
216.1
Origin
216.1.1 Spinous
processes of 1st -Sth thoracic vertebrae
216.2
Insertion
216.2.1 Superior
border of spine of scapula
216.3
Action
216.3.1 Retracts
and aids in elevation of scapula
216.4
Nerve Supply
216.4.1 Spinal
accessory and ventral rami, C3, 4
216.5
Synergists
216.5.1 Rhomboids,
levator scapulae, upper and lower divisions of trapezius
216.6
Category
216.6.1
216.7
View
216.7.1
Posterior View
217
TRAPEZIUS UPPER
217.1
Origin
217.1.1 External
occipital protuberance, medial 1/3 of superior nuchal line, ligamentum nuchae
and spinous process of the 7th cervical vertebra
217.2
Insertion
217.2.1 Lateral
1/3 of clavicle and acromion process
217.3
Action
217.3.1 Elevates
the scapula as in shrugging the shoulders. Rotates the scapula upwards so the
glenoid cavity faces superiorly, when acting with the other sections of the
trapezius it retracts the scapula. REVERSED ORIGIN-INSERTION ACTION: Laterally
flexes head and neck to side of contraction. Rotates head and neck away from
side of contraction. Acting bilaterally, extends the head and neck
217.4
Nerve Supply
217.4.1 Spinal
accessory and ventral rami of C3, 4
217.5
Synergists
217.5.1 Levator
scapulae, clavicular head of the ster- nocleidomastoid, middle and lower
trapezius
217.6
Category
217.6.1
217.7
View
217.7.1
Posterior View
218
TRICEPS BRACHII
218.1
Origin
218.1.1 LONG
HEAD: Infraglenoid tubercle of scapula. LATERAL HEAD: Superior 1/2 of posterior
lateral surface of humerus. MEDIAL HEAD: Inferior '2/3 on the posterior surface
of the humerus
218.2
Insertion
218.2.1 Supraposterior
surface of the olecranon process of the ulna and deep fascia of the forearm
218.3
Action
218.3.1 Extends
forearm at the elbow. Long head aids in adduc- tion and extension of the arm at
the shoulder
218.4
Nerve Supply
218.4.1 Radial,
C6, 7, 8, with separate branches for each head
218.5
Synergists
218.5.1 Anconeus
218.6
Category
218.6.1
218.7
View
218.7.1
Posterior
View
219
URETHRAL SPHINCTER
219.1
Origin
219.1.1
219.2
Insertion
219.2.1
219.3
Action
219.3.1
219.4
Nerve Supply
219.4.1
219.5
Synergists
219.5.1
219.6
Category
219.6.1